According to the most recent year of data available, an estimated 42% of adults have obesity and almost 20% of children are diagnosed with obesity. It is well documented that obesity prevalence and associated health care costs continue to rise. The Kaiser Family Foundation has estimated the average annual health spending for people enrolled in commercial insurance diagnosed with obesity grew from $9,500 in 2011 to $12,500 in 2021, over 1.5 times higher than people not diagnosed with obesity.
Additionally, people with obesity are at increased risk for other diseases and chronic conditions. Among people with employer-sponsored insurance (ESI) in HCCI’s dataset and people enrolled in Medicaid, the most common comorbidities among people diagnosed with obesity were dyslipidemia (abnormal levels of fats like high cholesterol), diabetes, and depression.
Historically, obesity has been treated with lifestyle interventions, such as nutrition therapy and behavioral counseling, and gastric bypass or sleeves procedures. More recently, people with obesity are being prescribed anti-obesity medications (AOMs). Medications, like semaglutides, that were originally prescribed for diabetes patients are now being approved to treat obesity.
In this brief, we analyze the frequency of obesity treatments in 2021 and 2022 using HCCI’s claims dataset of people who get insurance through work and Medicaid (T-MSIS) data. Overall, anti-obesity medications are the most common treatment among people with ESI. Lifestyle interventions are the most common treatment among people with Medicaid. Among young people (under age 25) with both types of insurance, lifestyle interventions are the most common treatment. Lifestyle interventions and bariatric surgery are most likely to be used among age groups 25-34 and 35-44 while AOMs are most commonly used among ages 45-54. Our analysis also shows that women are more likely than men to be prescribed any treatment for obesity. Utilization of all obesity treatments vary by state, which can be explored in detail in the map below.
People with ESI, women, and people between the ages of 45 and 54 are most likely to treat diagnosed obesity with Anti-Obesity Medications
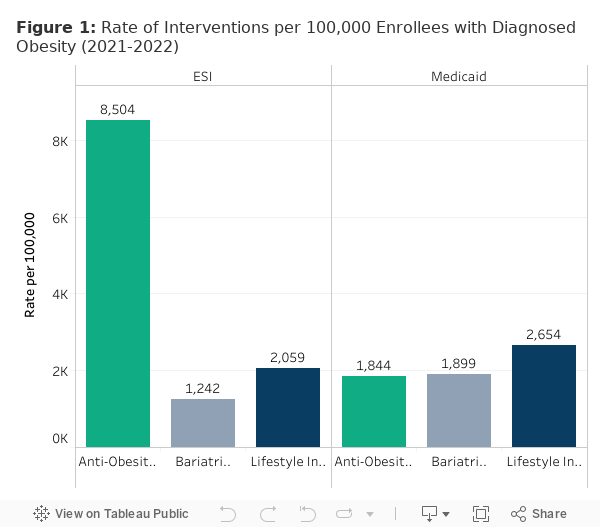
The most common obesity treatment among the ESI population diagnosed with obesity, AOMs were prescribed to just over 8,500 per 100,000 enrollees in 2021 and 2022. In contrast, approximately 1,800 per 100,000 Medicaid enrollees received AOM treatment. Lower AOM utilization rates among the Medicaid population is likely due to varying Medicaid drug coverage policies by state.
Women were more likely to be prescribed AOMs than men. Women enrolled in ESI received AOMs at nearly twice the rate of men (about 11,000 per 100,000 compared to 5,550 per 100,000, respectively). In Medicaid, fewer people were prescribed AOMs, but women still received them at twice the rate of men. Women with Medicaid received AOMs at a rate of about 2,300 per 100,000 compared to 1,150 per 100,000 male enrollees.
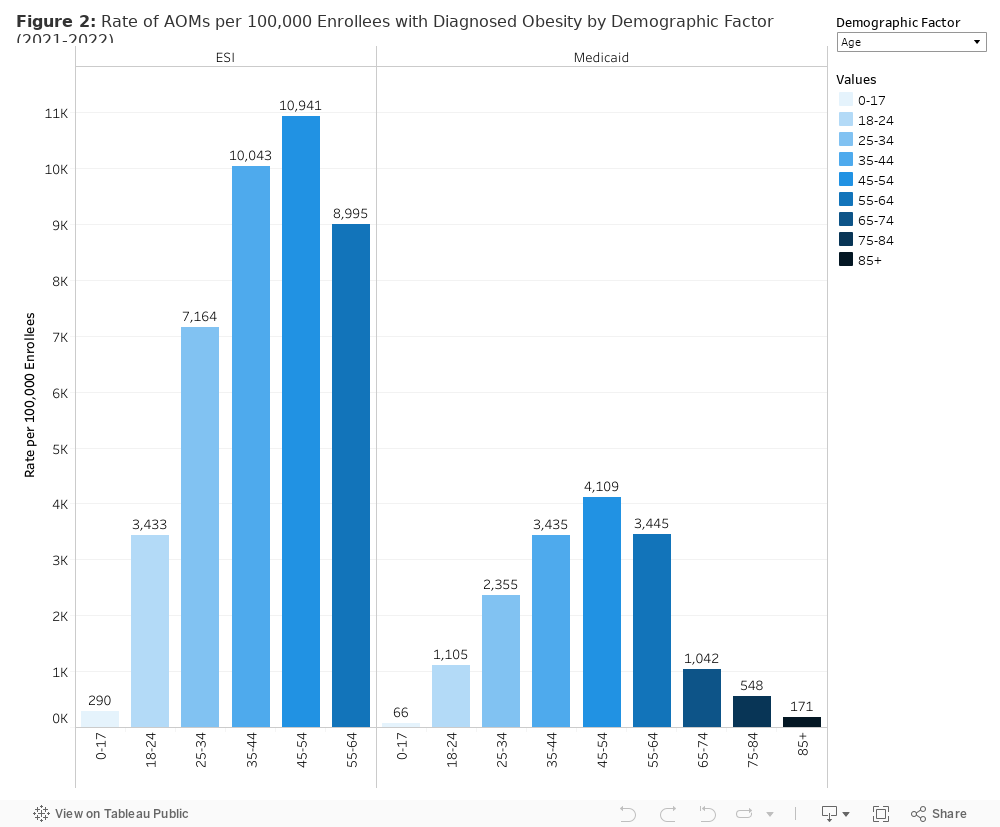
People between the ages of 45 and 54 with diagnosed obesity were more likely than other age groups to use AOMs. Among people with ESI, nearly 11,000 per 100,000 enrollees 45-54 were prescribed AOMs, and approximately 4,100 per 100,000 Medicaid enrollees in this age group were prescribed AOMs.
Within the ESI population, except for children under the age of 18, each age group in our analysis with diagnosed obesity was more likely to be treated with AOMs than any other intervention. For example, people between the ages of 25-34 were nearly three times more likely to be prescribed an AOM than to receive a lifestyle intervention. ESI enrollees 45-54 were seven times more likely to receive an AOM than bariatric procedures and twice as likely to receive AOMs than lifestyle intervention.
Children under the age of 18 had the lowest rates of AOM use. Around 300 per 100,000 ESI enrollees were prescribed AOMs, almost four times higher than Medicaid enrollees (over 60 per 100,000 enrollees). The American Academy of Pediatrics has said that there is insufficient evidence to recommend use of AOMs to children 12 years or younger, which could contribute to lower rates of use among children. Liraglutides, like Saxenda®, and some semaglutides (Wegovy®) are approved for children 12 and older but not all semaglutides, like Ozempic®, are approved for children under 18.
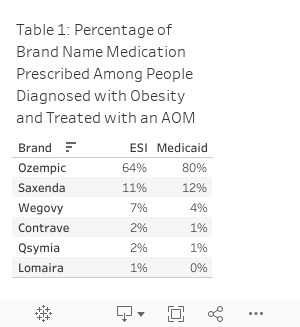
In 2021 and 2022, the most commonly prescribed AOM in both ESI and Medicaid was Ozempic ®, a semaglutide approved by the FDA to treat type 2 diabetes. Perhaps because people with obesity frequently also had a diabetes diagnosis, nearly two-thirds of people diagnosed with obesity with ESI who were prescribed an AOM were prescribed Ozempic®. In Medicaid, 80% of people diagnosed with obesity using an AOM were prescribed Ozempic®. The next most prescribed brand was Saxenda®, (11% in the ESI population and 12% in the Medicaid population), followed by Wegovy® (7% of ESI AOM prescriptions, 4% of Medicaid AOM prescriptions).
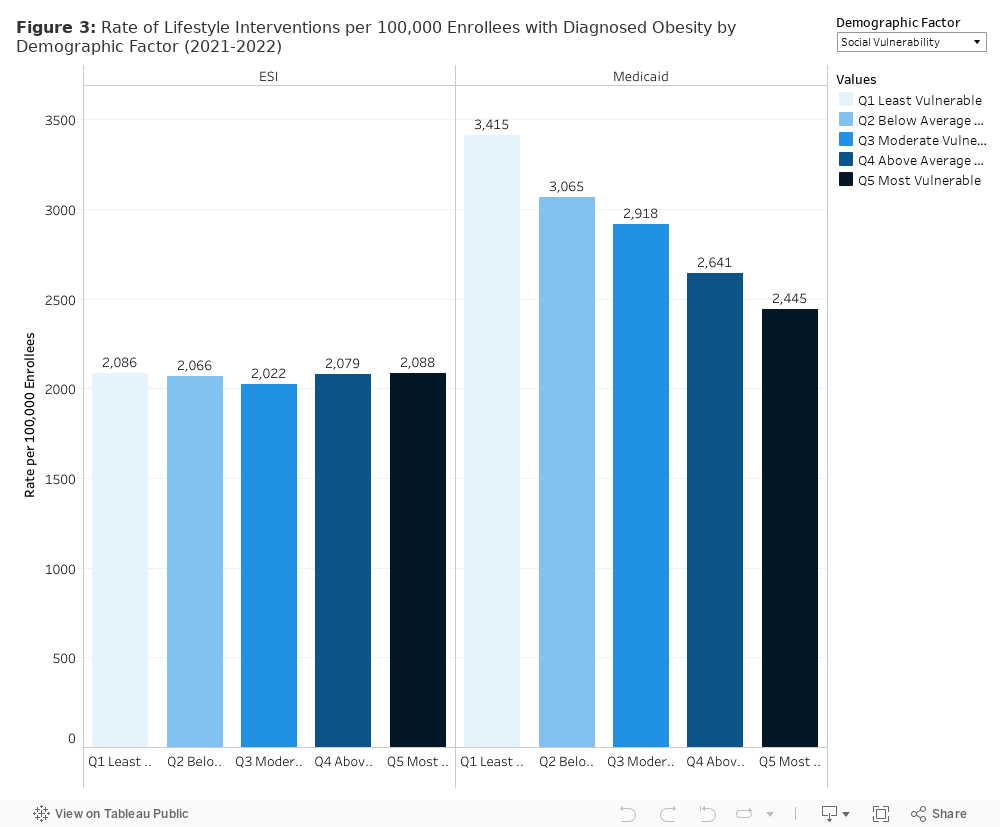
Rates of lifestyle interventions are similar among payer populations
Overall, lifestyle intervention was the second most common treatment for obesity among people enrolled in ESI and Medicaid. We observed slightly higher treatment rates of lifestyle interventions among people with Medicaid (about 2,650 per 100,000 enrollees) compared to people with ESI (approximately 2,000 per 100,000 enrollees). Lifestyle intervention was the most common obesity treatment among children under 18 enrolled in both ESI and Medicaid who used lifestyle interventions at similar rates (approximately 1,400 per 100,000 enrollees).
Although women were more likely to use at least one lifestyle intervention than men, the gap was smaller than for AOMs or bariatric procedures. Approximately 2,700 per 100,000 women with ESI used at least one lifestyle intervention, nearly double the rate of 1,365 per 100,000 among men with ESI. Women with Medicaid used at least one lifestyle intervention at a rate of about 3,200 per 100,000 compared to 1,800 per 100,000 among male enrollees.
In both Medicaid and ESI, people with obesity between the ages of 25 and 34 years old and 35 and 44 used lifestyle interventions at the highest rates. Even within these age bands, lifestyle intervention was more common among people with Medicaid than ESI. For example, 25-34 year olds with Medicaid used lifestyle intervention at a rate of 4,800 per 100,000, over 1.5 times higher than people with ESI (2,900 per 100,000 enrollees). People with obesity ages 35-44 enrolled in ESI used lifestyle interventions at a rate of about 2,600 per 100,000 enrollees and people enrolled in Medicaid used lifestyle interventions at a rate of 4,300 per 100,000 enrollees. The third highest age group was people ages 45-54 who used lifestyle interventions at a rate of 2,100 per 100,000 ESI enrollees and around 3,400 per 100,000 Medicaid enrollees.
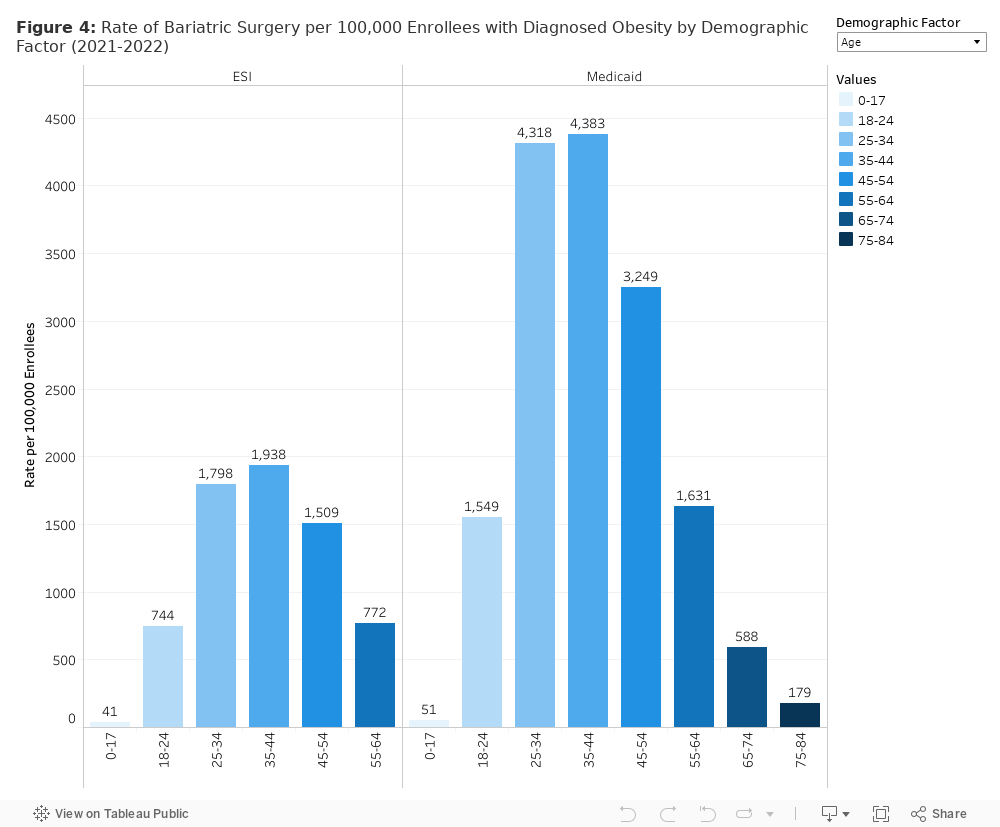
Bariatric surgery is more common among Medicaid enrollees than among people with ESI
The rate of bariatric surgery among people enrolled in Medicaid is higher than people with ESI (about 1,900 per 100,000 enrollees and 1,200 per 100,000 enrollees, respectively). In part, this could be because the Affordable Care Act expanded Medicaid coverage for the procedure, and studies have shown that this was correlated with an increase in bariatric surgeries.
Among people with ESI and Medicaid, women were significantly more likely than their male counterparts to have a bariatric procedure. Women enrolled in ESI were 3.5 times more likely to receive bariatric surgery than men (1,860 per 100,000 enrollees and 530 per 100,000 enrollees, respectively). In Medicaid, approximately 2,700 women per 100,000 had bariatric surgery compared to 595 per 100,000 male enrollees.
As with lifestyle interventions, bariatric surgery use was highest among enrollees between 25 and 34 years old and between 35 and 44 years old for both ESI and Medicaid. Rates of bariatric surgery were higher among people with Medicaid at every age band studied. For example, the rate of bariatric surgery for ESI enrollees between 25 and 34 years old was nearly 1,800 per 100,000 enrollees and 4,300 per 100,000 Medicaid enrollees. Among people aged 35-44, the rate of bariatric surgery for people with ESI was almost 2,000 per 100,000 enrollees. The Medicaid rate was over twice as high at 4,400 per 100,000 enrollees. The rate of bariatric surgery among children with diagnosed obesity was extremely low among people with ESI and Medicaid. The American Academy of Pediatrics only recently included bariatric surgery in their treatment guidelines and still some hospitals do not perform bariatric surgery on children under 18.
Obesity Treatment Differs between ESI and Medicaid
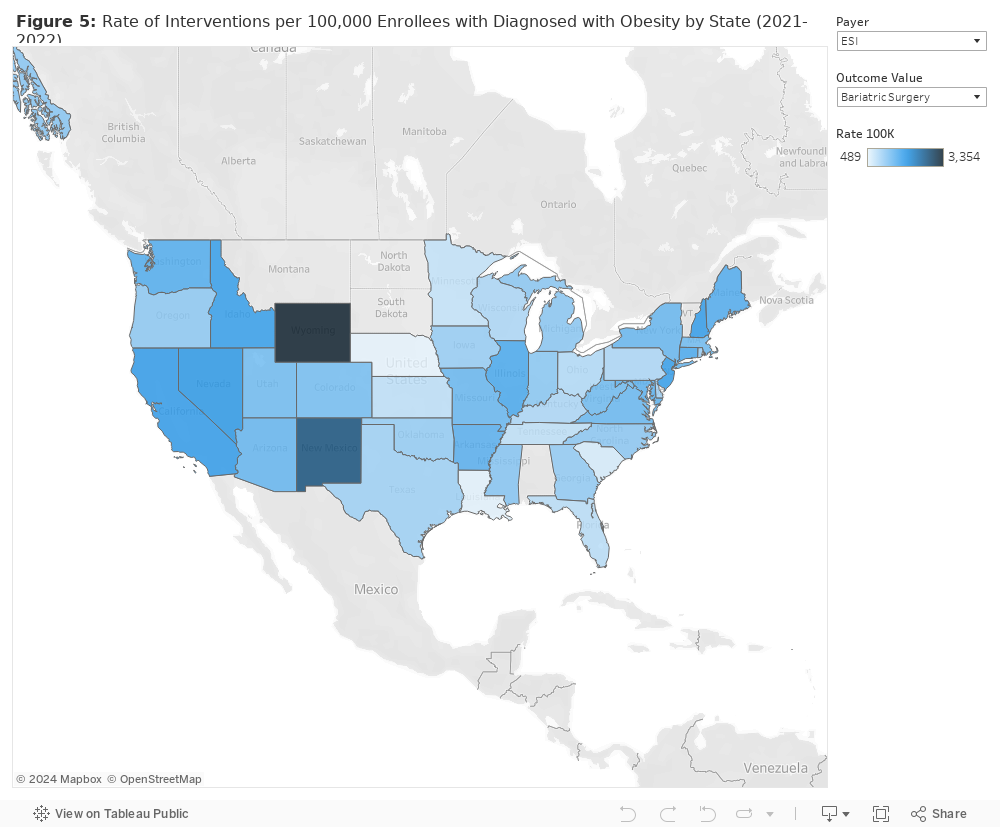
Our analysis shows that treatment patterns for obesity vary between the Medicaid and ESI populations. The rate of lifestyle interventions to treat diagnosed obesity is similar, but AOM use is far more common among people with ESI while bariatric surgery is more common among people with Medicaid. In both ESI and Medicaid, our data show higher use of all treatment interventions among women compared to their male counterparts. AOMs were more common among adults ages 45-54 years old while bariatric surgery and lifestyle interventions were a more common treatment for adults ages 25-34 and 35-44. Differences in health care coverage policies between ESI and Medicaid, including differences in Medicaid coverage among states, likely contribute to the differences we see. We observe a wide variation of the rates of each intervention by state among both people with Medicaid and ESI [Figure 5]. Clinical guidelines regarding the appropriateness of certain treatments (i.e., AOM and bariatric procedures) also may affect the observed patterns. The focus on treating obesity, particularly AOMs, is intensifying. As public and private policymakers work to address this critical public health challenge, this analysis illustrates current practice patterns and the impact of policies guiding treatment.
Methodology Note
Our ESI cohort includes beneficiaries who were continuously enrolled in an ESI plan with prescription drug coverage for all of 2021-2022. Our Medicaid cohort includes beneficiaries who were continuously enrolled in either Medicaid or CHIP for the same time period. For these cohorts, we pulled all inpatient, outpatient, and physician claims to look for claims with at least one claim with severe obesity in any diagnostic position. A limitation of this study is that the prevalence of obesity among our sample is lower than the national estimate from NHANES data likely due to under coding of obesity diagnosis codes in administrative claims data. To identify patients with comorbidities, we used claims data with at least one claim in any diagnostic position (using the definitions from AHRQ’s Clinical Classification Software Refined). To identify rates of gastric surgeries, we pulled inpatient, outpatient, and physician claims to identify patients with a CPT or DRG code listed in previously published studies (Kan et. al. and Amman et. al). Note, some hospitals require patients to have a BMI of 35kg/m2 or higher to be considered for bariatric surgery and health plans vary in BMI requirements in order to be covered.We used the same method to identify lifestyle interventions (Kan et. al). To be included as a lifestyle intervention, the patient had to have an obesity diagnosis on the same claim. To identify rates of anti-obesity medication use, we pulled pharmacy claims with an NDC in Milliman’s list of AOMs. To categorize patients into social vulnerability levels, we used HHS’ SVI composite index.