In HCCI’s most recent Health Care Cost and Utilization Report, we observed substantial growth in spending on vaccines among individuals with employer-sponsored health insurance (ESI), which we attributed largely to uptake of COVID-19 vaccinations in 2021. Although they may be largely responsible for this trend, federal procurement complicates analyses of COVID-19 vaccines using claims data. Researchers interested in studying uptake and total and out-of-pocket costs of COVID-19 vaccines using claims data should be aware of changes in billing patterns brought on by federal pandemic policies.
Traditionally, claims for routine vaccinations consist of two components: the vaccine itself and the administration of the vaccine. Insurers and health care providers typically negotiate with manufacturers to purchase the supply of vaccine they need. As part of the COVID-19 vaccine rollout in late 2020, the federal government negotiated directly with manufacturers to purchase a national supply of COVID-19 vaccines in a departure from the existing system. The federal government then distributed the COVID-19 vaccines to pharmacies and provider offices without cost to health care providers.
These changes to vaccine procurement led to billing changes in COVID-19 vaccine claims, complicating correct identification of COVID-19 vaccine use. To assess the implication of these pandemic policies for analysis of COVID-19 vaccines in claims data, we compared the claims billing patterns of COVID-19 to those of standard influenza vaccines by site of care (e.g., pharmacy versus doctor’s office) among ESI enrollees in HCCI’s claims database in 2021.
Due to Federal Vaccine Procurement, the Majority of COVID-19 Vaccine Claims Do Not Include the Vaccine Itself
Because the federal government purchased COVID-19 vaccines directly and distributed them to providers at no cost, providers were not allowed to receive reimbursement for the COVID-19 vaccines from insurers. Accordingly, despite valid CPT codes and COVID-19 vaccine billing guidelines released by CMS, we found that the majority of COVID-19 vaccine administrations claims in 2021 did not have an associated claim for the vaccine itself. Specifically, only 25% of the COVID vaccine administration claims occurring in doctors’ offices had claims for both the administration and the vaccine billed by providers for reimbursement (Table 1).
In contrast, since influenza vaccines are procured directly by providers, over 90% of all flu vaccine claims in doctors’ offices in 2021 had both an administration and vaccine code billed by providers for reimbursement.
In the absence of COVID-19 vaccine codes in physician office claims, researchers can rely on COVID-19 vaccine administration CPT codes to identify both the specific COVID-19 vaccine product and dosage (e.g., first dose, second dose, or booster). If the research question requires the complete cost of COVID-19 vaccine administration, researchers should be aware that most of the reimbursed amounts in claims are missing the cost of the actual vaccine itself.
Table 1. Presence of Vaccine and Administrations Claims for COVID-19 and Flu Vaccines, 2021
| Influenza | COVID-19 | |
| Vaccine and Administration | 90.9% | 26.0% |
| No Vaccine and Administration | 9.1% | 74.1% |
Pharmacies Administered the Majority of COVID-19 Vaccines Among ESI Enrollees in 2021
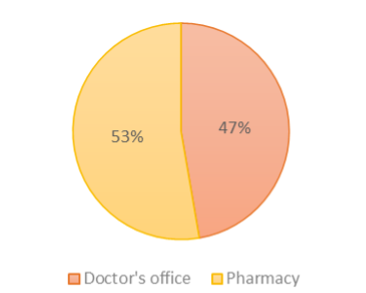
We found that 53% of all COVID-19 vaccine administrations among ESI enrollees were administered in pharmacies in 2021, reflecting their leading role in COVID-19 vaccine rollouts in most states. In comparison, we found that just 17% of all flu vaccines among ESI enrollees were administered in pharmacies in 2021.
Claims for COVID-19 vaccines administered in pharmacies are adjudicated under the pharmacy benefit while claims for COVID-19 vaccines administered in doctors’ offices are adjudicated under the medical benefit. Therefore, researchers using administrative claims data to study COVID-19 vaccines should use both medical and pharmacy claims (vaccines identified through National Drug Codes) for data completeness. A limitation of vaccines billed through pharmacy is the inability to separate vaccine costs from administration costs.
Figure 1. Site of COVID-19 Vaccine Administration in 2021
Implications for Tracking of COVID-19 Vaccines in Administrative Claims Data
The federal government’s decision to negotiate and purchase COVID-19 vaccines directly on behalf of the nation altered private insurance billing practices for COVID-19 vaccines. Billing practices for COVID-19 vaccines may change again when the current COVID-19 drug stockpile becomes depleted and providers revert to purchasing their own vaccine supply as they have done historically.
Researchers using administrative claims data to study COVID-19 vaccines or related services should consider temporal changes in claims billing patterns resulting from federal policy changes. Moreover, claims-based analysis of COVID-19 and flu vaccines will likely underreport how many people have received the vaccine given opportunities to receive vaccines through state, city, employer, and other initiatives that may not have resulted in an individual insurance claim. Still, understanding the total and out-of-pocket burdens associated with vaccine provision is an important component of public health and health policy efforts to reduce infectious disease and improve health care provision.