
Since the onset of the COVID-19 pandemic, a growing body of research has found alarming disparities in rates of the virus among Black and Hispanic communities. For example, the CDC reports that “American Indian or Alaska Native, Non-Hispanic” people and “Hispanic or Latino” people each have 2.8 times as many COVID cases than white people, Black patients have 2.6 time as many, and Asian people have 1.1 times as many COVID cases as white patients. Previous HCCI analysis found that Hispanic and Black patients were more likely to test positive for COVID and COVID antibodies than non-Hispanic white patients; Hispanic patients were approximately four times more likely to test positive for COVID and over six times more likely to test positive for antibodies compared to white patients, and Black patients were twice as likely to test positive for COVID and over three times more likely to test positive for COVID antibodies than white patients.
This analysis built on that research and found that the trends persisted. Specifically, disparities in positivity rates, measured as the percentage of COVID test and COVID antibody tests (collectively referred to as “COVID tests”) that were positive out of all COVID tests in our data, continue across two unique regions of the US that have experienced dramatic increases in COVID cases at different times. The NY Tri-State region (Connecticut, New Jersey, and New York) had many more COVID cases in the initial phases of the pandemic with New York City and its surrounding areas are widely held as the epicenter of the pandemic in the US at the end of March and through April. In contrast, the Deep South region (Alabama, Arkansas, Louisiana, and Mississippi) experienced more cases over the summer and even into the Fall.
We studied records from an ambulatory electronic medical record data platform with data from over two hundred community health centers, primary care, immediate/urgent care, and specialty care providers serving 20 million unique patients. In both regions, we found that Hispanic and Black patients have higher rates of infection than white patients. Although the patterns change over time, over most of the study period, we observed a greater disparity between Hispanic patients and white patients than between Black patients and white patients.
National positivity rates were consistent with anecdotal reports of COVID-19 spread.
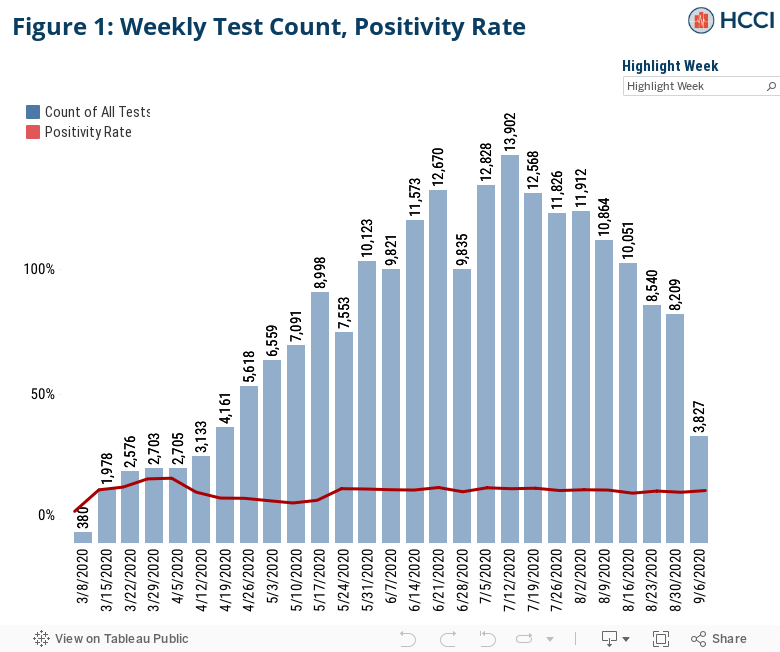
We analyzed data from March 8, 2020 through the week of September 6, 2020 to understand the impact of COVID-19 on patients seeing these providers. Figure 1 shows the total number of COVID tests administered by all providers in our sample and the positivity rate.
In the second week of March, 368 COVID tests were performed, with subsequent weeks averaging just over 2,000 tests per-week, and a positivity rate up to 17 percent, consistent with reporting on the initial wave of the pandemic. Thereafter, the number of COVID tests administered rose rapidly and the positivity rate fell, reaching over 10,000 tests administered per week in June and July and a positivity rate of about 12 percent. Since mid-July, administered tests have decreased among providers in our sample, dropping to about 3,000 in the first week of September. The decline may be a function of the convenience sample itself, and not representative of the experience of the ambulatory care population. While we expected the number of administered tests to have continued increasing, the data we see may be a result of patients finding increasing alternatives for testing, such as county health sites, which are not included as part of our sample. Despite the recent drop in tests, the positivity rate has remained constant since late May, at 12 percent.
Regional positivity rates were consistent with anecdotal reports of COVID-19 spread.
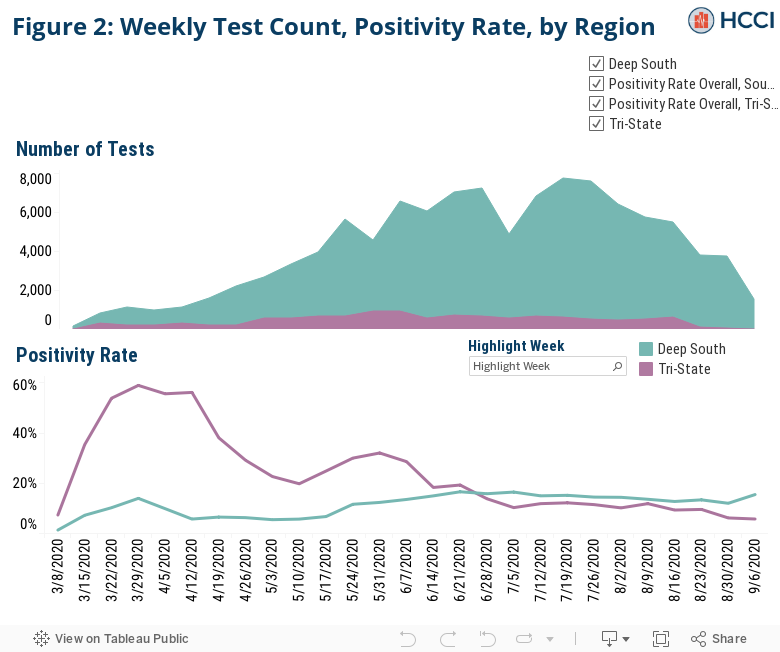
Figure 2 shows the number of tests administered and the positivity rate COVID tests by the two regions in this study. Across our sample, positivity rates peaked at 17 percent in early April, before levelling off at approximately 12 percent for the rest of the period studied. In the Tri-State region, positive COVID tests were significantly higher in the initial months of our analysis, reflecting the significant toll the pandemic has had on the Tri-State region. Positive COVID tests peaked at almost 60percent in early April before becoming more consistent with overall trends in our sample by mid-summer. In the Deep South, however, positivity rates gradually increased over the course of the summer peaking at 17 percent in late June and exceeding positivity rates in the Tri-State region for much of the summer. For more details on our data and methods please refer to the Methods section of our earlier report.
Disparities in positivity rates persist over time and across geography.
As noted above, HCCI’s earlier research found that Hispanic and Black patients were more likely to have positive COVID tests than white patients. This analysis found those higher positivity rates in both regions studied and over time. Figure 3 presents the positivity rate among Hispanic, Black, and white patients in the two regions studied.
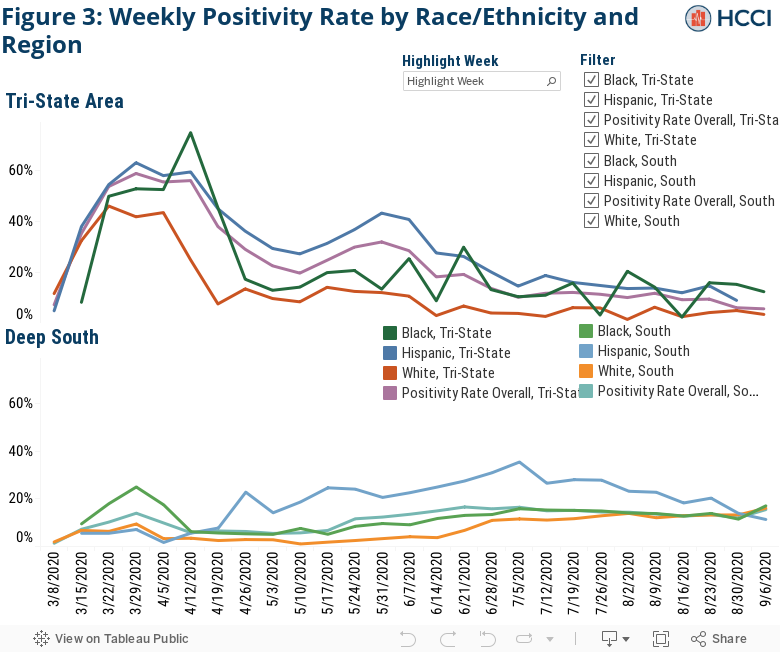
The positivity rate among both Hispanic and Black patients in the Tri-State region was significantly higher than that of white patients throughout the study period. In mid-April, the positivity rate among Hispanic patients was almost six times higher than that of white patients (e.g., 45 percent versus 8 percent for the week of April 19). At the same time, the same was true in the incidence of positive tests for Black patients vs white patients. Since the beginning of June, in the Tri-State region, the positivity rate among Hispanic patients has been trending down, though remains three to four times higher than that of white patients and the positivity rate among Black patients generally has been more than twice the rate of white patients. We observed volatility towards the end of the study period, likely caused by the smaller number of tests described above.
In the Deep South, from mid-April through early July, the percent of positive COVID tests for Hispanic patients was more than three times the positivity rate for white patients. Despite several weeks in March in which the positivity rate among Hispanic patients was lower than white patients, early in the study period, in mid- May, the positivity rate among Hispanic patients was more than 12 times higher than among white patients. Also, early in the study period, the gap in the positivity rate between Black patients and white patients dramatically exceeded the disparity between Hispanic patients and white patients. Since early April, Black patients in the Deep South have been more likely to have a positive COVID test than white patients, frequently with positivity rates two to three times larger than white patients. However, at the beginning of August, Black and white patients had similar positivity rates, around 13 percent. This is the first time in the data that we see this the racial disparity shrink.
Hispanic patients were disproportionately more likely to test positive for COVID across regions. Our earlier study found that, across our sample, Hispanic patients accounted for 16 percent of COVID tests but represented almost half of positive COVID tests. In other words, Hispanic patients were much more likely to test positive for COVID and antibodies than white patients. In this analysis, we found that the disparity in COVID positivity rates persisted across both geographic regions we studied.
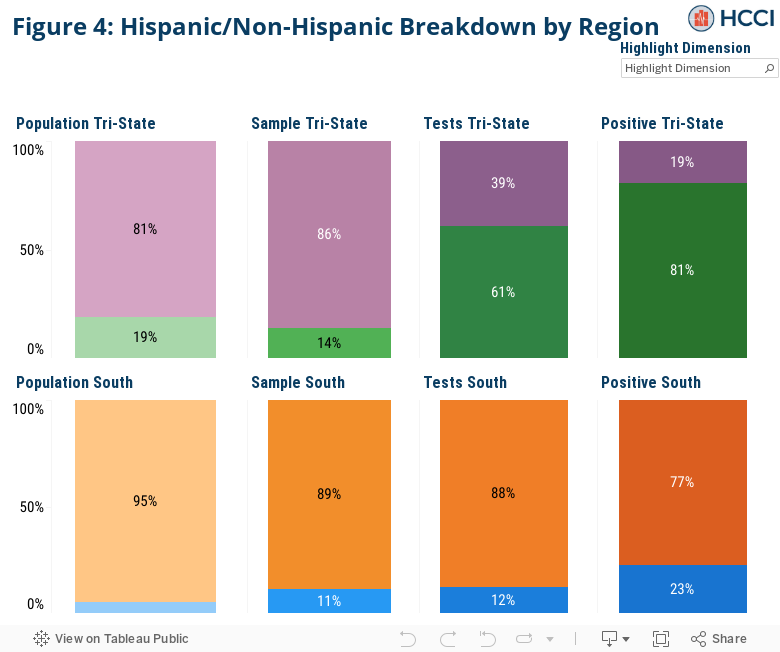
In the Tri-State region, Hispanic patients made up 14 percent of the study population but 58 percent of COVID tests and 81 percent of positive COVID tests. As shown in Figure 4, Hispanic people made up 19 percent of the total population in the Tri-State region, according to American Community Survey 2018 data. In 2019, our Tri-State area sample of providers saw nearly 450,000 unique patients, of which 14 percent identified as Hispanic. Hispanic patients made up 61 percent of patients tested by the end of August 2020 but accounted for 81 percent of the positive COVID tests.
In the Deep-South region, Hispanic patients made up 11 percent of the study population but 13 percent of COVID tests and 26 percent of positive COVID tests. Figure 4 shows that Hispanics made up 5 percent of the total population in the Deep South states, according to American Community Survey 2018 data. In 2019, our providers in the Deep South saw almost 1.4 million unique patients, of which 11 percent identified as Hispanic, yet Hispanic patients accounted for 12 percent of COVID tests and 23 percent of the region’s positivity rate. Although these differences are not quite as pronounced as in the Tri–State region, they still are indicative of the disproportionate burden of COVID-19 on the Hispanic population.
Pandemic response needs to address disproportionate impact on Hispanic and Black communities.
The disproportionate burden of disease on Hispanic/Latino and Black communities reflect greater social and economic disparities built on a foundation of racism and discrimination. For example, according to the New York Times, 43 percent of Black and Latino workers are employed in service or production jobs that for the most part cannot be done remotely, compared to around 25 percent of white workers. These jobs often put workers at a higher risk of exposure to COVID. In addition, crowded living conditions and multi-generational households, both more common in Black and Latino/Hispanic communities than in white communities, further the risk of infection to COVID. When compared to their white counterparts, the systemic lack of economic opportunities, and of access to health care, among other unjust social determinants of health, creates inequalities that make Black and Latino/Hispanic people more vulnerable to, and more likely to die from, this virus.
Reporting and other research have consistently identified the heavier burden COVID has placed on Hispanic and Black communities. We found similar disparities in this analysis. In both the Tri-State and Deep-South regions, Hispanic and Black patients consistently had higher rates of positive COVID tests than white patients over the study period. As the country continues to reckon with the impact of the pandemic, it seems increasingly clear that solutions will need to address the inequities in the disease burden in Black and Hispanic communities. Public health efforts at regional and local levels should address the needs of the communities most impacted by the pandemic. This report aims to highlight the incidence of COVID using data from ambulatory electric medical records supplementing information more typically collected from departments of health. We hope policymakers will use this and other research to pursue evidence-based interventions to mitigate the spread of the disease and to address the dramatic and disproportionate impact of COVID on Black and Hispanic communities.
Methods Note
We examined laboratory orders from a convenience sample of electronic medical records1 provided by a data management platform vendor with order dates beginning March 8, 2020. Our unit of analysis is a unique “patient laboratory order” + “order date” which means a patient who gets tested more than once on different days may appear in the data more than once. The data cover orders from over 4 million patients seen by over 200 group practices or clinics for all patients seen by the practice or clinic regardless of payer type. The majority of encounters on the laboratory order were classified as an office visit.
We divided the data into two U.S. regions. Table 1 shows the states included in each region and are based on the patient’s address.
Table 1. Distribution of All Tests Administered (COVID and Antibody) by U.S. Region
| Region | States |
| Deep South | Arkansas, Mississippi, Louisiana, Alabama |
| Tri-State | New York, New Jersey, and Connecticut |
Using a series of regular expression queries, we searched for two types of tests that are used to determine COVID-19 infection. We identified PCR tests (“COVID test”) that are used to determine whether a patient currently has the virus that causes COVID-19, and we identified blood serum antibody tests (“antibody test”) that are used to help determine if a patient has previously been infected with the virus that causes COVID-19. Key search terms were compiled from a list of COVID-19 PCR and COVID-19 antibody test descriptions at the FDA, and can be found here. For this analysis, we did not differentiate results based on the type of test conducted (COVID vs antibody). We also used regular expressions to determine which tests returned a positive result; these were gathered from the EMR test notes. The percent positive is based on the number of positive tests among all tests, not just the ones with a known result.
There are a few limitations to this analysis. This data comes from a convenience sample of ambulatory care providers. As such, we do not capture a representative sample of all tests administered in our study regions, nor all of the tests that would be recorded by public health departments. While the percent positive rate is roughly similar to data released by the CDC (see: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html), we do see a greater drop in administered tests than the CDC’s nationally reported figures. Additionally, we use race and ethnicity data reported on the electronic medical record, which previous research indicates may underreport Hispanic ethnicity and black race (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4441665/). Caution should be used in interpreting the results as the data may miss categorize some patient’s race and/or ethnicity.
1Electronic medical record (EMR) data including diagnosis, procedures, labs, vitals, medications and histories sourced from a data management platform vendor with EMR data on 40 million unique patients, updated daily. The data, technology, and services used in the generation of these research findings were generously supplied pro bono by the COVID-19 Research Database partners, who are acknowledged at https://covid19researchdatabase.org/.