Surgery accounts for the largest share of inpatient and outpatient spending among individuals with employer-sponsored insurance, representing 49 percent of inpatient spending and 37 percent of outpatient spending in 2018 according to HCCI’s most recent annual report. In recent years, the number of surgical procedures performed using robot assistance has increased dramatically. Intuitive, Inc., which produces the da Vinci surgical system, reports a nearly 3-fold increase in procedural volume from 2010 to 2017. Despite this increase, there has been little comparison of frequency, prices or outcomes associated with procedures that do and do not use robot assistance.
We used health care claims from the Health Care Cost Institute to examine the use of robot assistance for five surgical procedures: hysterectomies (inpatient and outpatient), kidney repairs/removals (inpatient), knee replacements (inpatient), prostatectomies (inpatient), and small/large bowel (inpatient) surgeries. Specifically, we calculated the share of each type of surgery that used robot assistance, spending per procedure, length of stay, and spending per day for inpatient admissions between 2013 and 2017. We observed that:
- Prostatectomies used robot assistance most often and knee replacements used robot assistance least often;
- The proportion of surgeries that used robot assistance increased between 2013 and 2017 for most of the procedures we examined;
- The difference in spending for procedures that used robot assistance compared to those that did not vary by type of surgery.;
- Across all inpatient we procedures examined, the length of stay following surgeries using robot assistance was lower than surgeries without robot assistance; and
- Spending per day for inpatient stays following surgeries that used robot assistance was higher than surgeries without robot assistance for all procedures we examined.
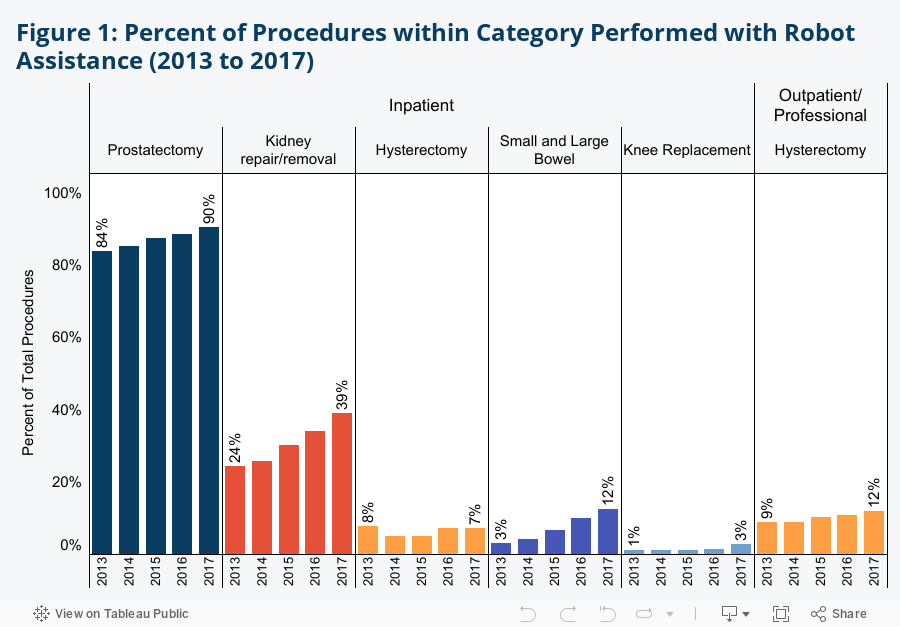
Share of Surgeries With Robot Assistance Was Higher in 2017 than in 2013.
The share of surgeries performed with robot assistance varied by procedure and generally increased during the study period. The share was highest for inpatient prostatectomies, increasing from 84 percent in 2013 to 90 percent in 2017. Inpatient knee replacement procedures used robot assistance least often, less than 5 percent of the time in each year between 2013 and 2017. The largest increases in the share of surgeries with robot assistance were seen in inpatient kidney repair/removal which grew from 24 percent in 2013 to 39 percent in 2017, and small and large bowel surgeries which grew from 3 percent in 2013 to 12 percent in 2017 (see Figure 1).
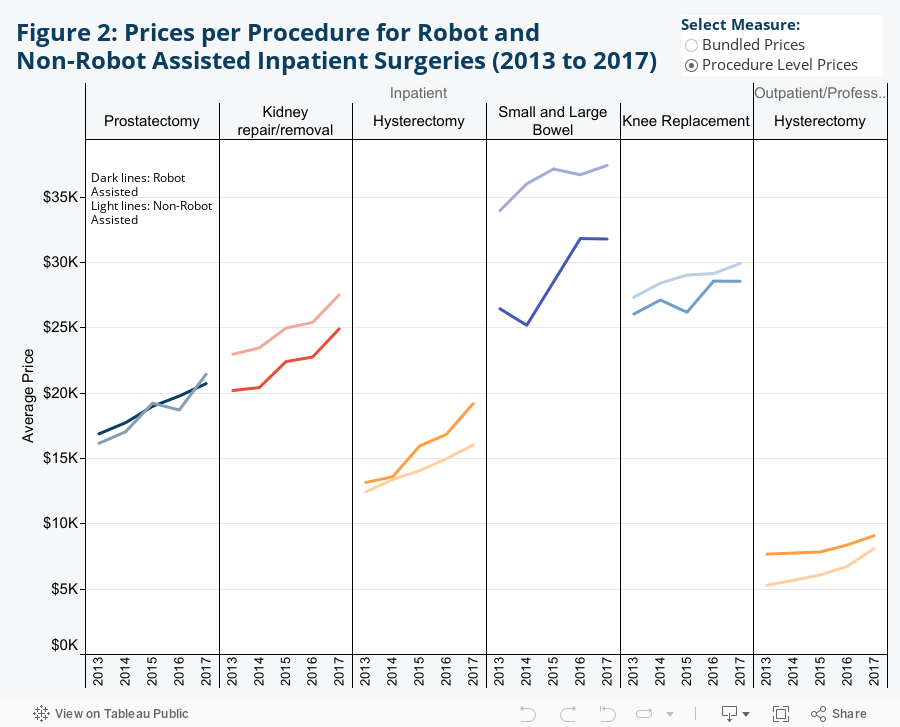
Spending for Robot-Assisted Procedures was Higher than Procedures without Robot Assistance for 2 of the 6 Procedures Studied
When we looked at spending per procedure for inpatient surgeries (by summing all claim lines associated with an inpatient admission), we found that spending per inpatient hysterectomy and outpatient hysterectomy were higher with robot assistance. In contrast, spending per inpatient kidney removal/repair, small or large bowel surgery, and knee replacement were lower with robot assistance. The average spending per prostatectomy with and without robot assistance was similar (see Figure 2). As we discuss in the limitations section, there may be differences across surgeries performed with and without robot assistance that explain some of the differences in spending, including shifts in procedures from the inpatient to the outpatient setting. Shifts from inpatient to outpatient settings may occur for many reasons, including patient preferences, clinical innovation, and financial incentives.
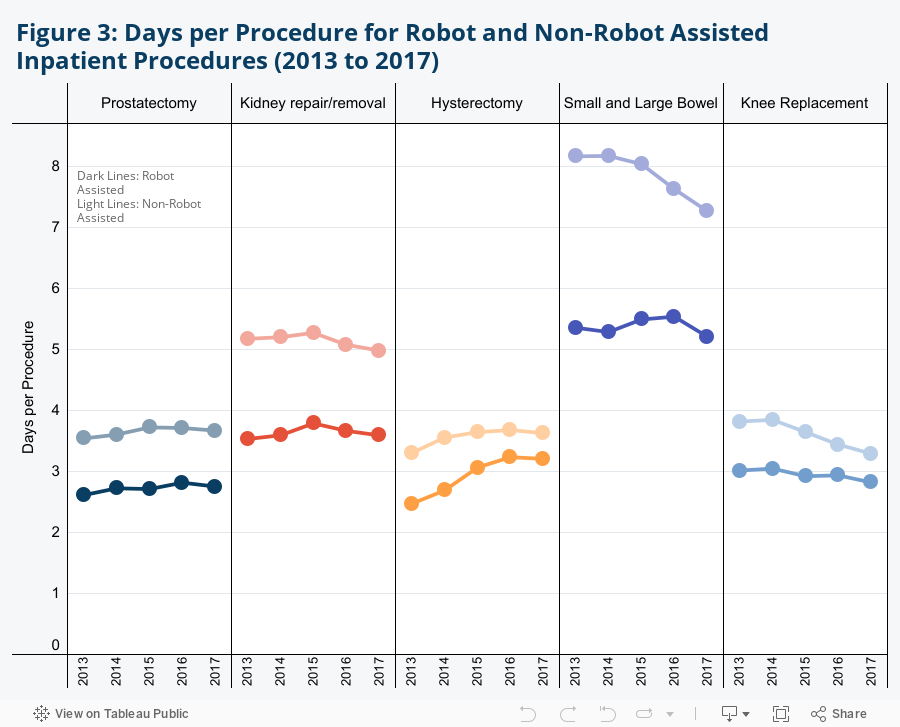
Length of Hospital Stay for Surgeries with Robot Assistance Was Shorter for all 5 Inpatient Procedures Studied
Following inpatient surgery with robot assistance, average hospital length of stay for individuals in our sample was 2.8 days for prostatectomies and 5.5 days for small/large bowel surgeries in 2017. This compares to 3.7 days and 7.3 days for prostatectomies and small/large bowel surgeries, respectively, performed without robot assistance in the same year (see Figure 3).
Over the study period, the difference in the average length of stay for surgeries performed with and without robot assistance decreased across most procedures we examined. In some cases, the average length of stay following surgeries performed without robot assistance declined (for example, small/large bowel surgeries and knee replacements), while for others the average length of stay following surgeries with robot assistance increased (inpatient hysterectomies). The changes we observe in length of stay for inpatient surgeries may also reflect shifts in site of service, changes in the composition of patients undergoing the particular type of surgery, or other changes in how the surgery is performed. In Appendix A we provide additional data on the share of surgeries performed in the inpatient and outpatient settings for each type of procedure.
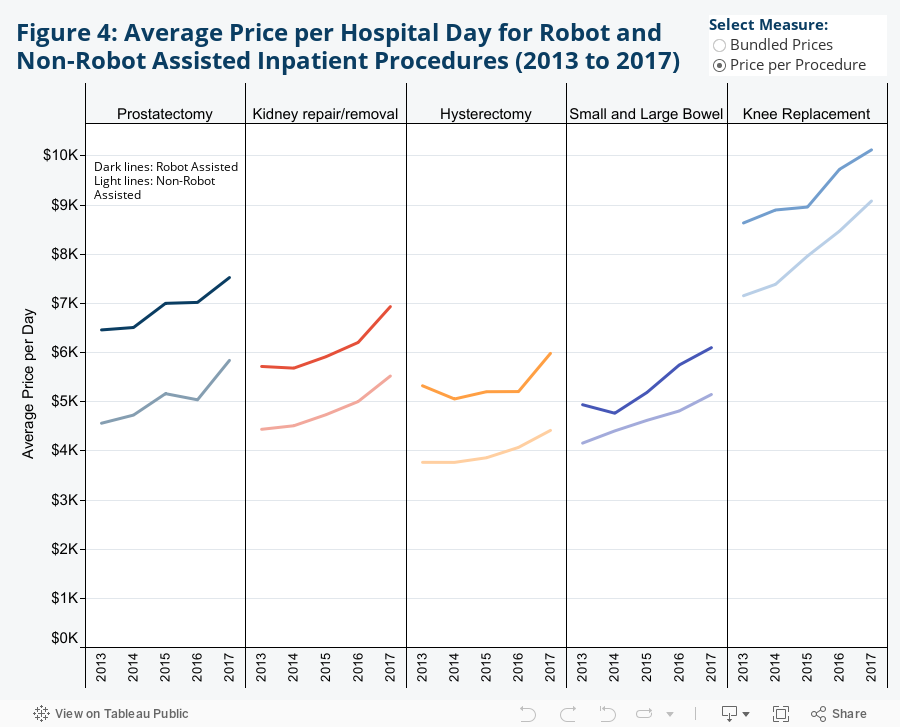
Robot-Assisted Procedures Had Higher Prices per Day
Given the differences in length of stay following inpatient surgeries with and without robot assistance, we calculated the spending per day for each procedure. We find that spending per day was higher when robot assistance was used for each of the procedures we examined. However, spending per day increased similarly across all procedures, regardless of the presence of robot assistance.
Conclusion
Innovation through new technology is believed to have many advantages, including reduced length of stay, lower medical errors, and other quality improvements. For example, robot-assisted surgery allows physician and non-physician providers to perform complex open and laparoscopic procedures via remote console. This new technology has been anecdotally reported to improve outcomes for patients and reduce physical demand on providers; this analysis does not attempt to measure outcomes. However, we believe that trends in utilization, spending per procedure, and length of stay among robot-assisted surgery may be of use to private and public policymakers as they consider the trade-offs in adopting new technology and innovation.
Limitations
The main limitation with this sort of analysis is the coding of robot-assisted procedures. In the inpatient setting, the use of ICD-9 and ICD-10 CM modifiers are used whereas the outpatient setting uses the CPT code of S2900. These coding practices give high sensitivity for determining that a robot was used in the procedure, but the specificity is not as high. This means this analysis accurately captures procedures where a robot was used, but it may undercount the total number of robot-assisted surgeries. This coding phenomenon is why common procedures such as hernia repair and cholecystectomy were not included; for example, the specificity issue is more pronounced in the outpatient setting, and since cholecystectomies and hernia repairs are rarely performed in the inpatient setting, they were not chosen as sentinel services. This analysis is meant to provide clarity around a subset of procedures which can be performed with robot assistance rather than give a broad view of all procedures that can be performed with robot assistance.
Although we examined surgeries to see if there were major differences in the gender and age of patients undergoing robot-assisted and non-robotic procedures (Appendices B and C), and found little difference between the 2 groups, the comorbidities, intensity, and other factors related to these 2 groups were not examined. These unobserved variables may affect the findings presented in the research.
HCCI data consists of over 40 million individuals per year with insurance sponsored by their employer, and for the purposes of this analysis, we limited the data to people aged 18-64. Although our data has a vast number of individuals in this category, it should not be utilized as a comprehensive sample for individuals who meet these criteria.
Methods Note
We analyzed a sample of individuals with employer-sponsored insurance aged 18-64 in HCCI’s vast claims database from 2013 to 2017. We excluded certain individuals to increase the certainty of the metrics reported for this brief. People who were enrolled in multiple health plans or moved between metro areas within a month were excluded. Claims with inpatient lengths of stay over 180 days or outpatient/professional lengths of stay over 2 days were excluded. Claims with no DRG, CPT, or HCPCS code on the claim line level were excluded. Individuals with unknown age and gender were excluded.
After preliminary exclusions, we then limited the sample to individuals who had one of six identified procedures: prostatectomies, kidney repairs/removals, hysterectomies, small and large bowel surgeries, and knee replacements. Procedures were classified into the six categories based on the following DRG and CPT codes:
| Inpatient DRG List for Included Procedures | ||||||
| Procedure | DRG List | |||||
| Prostatectomies | 707 | 708 | ||||
| Hysterectomies | 740 | 741 | 742 | 743 | ||
| Kidney Repairs/Removals | 656 | 657 | 658 | 659 | 660 | 661 |
| Small and Large Bowel Surgeries | 329 | 330 | 331 | |||
| Knee Replacements | 469 | 470 | ||||
| Outpatient CPT List for Included Procedures | ||||||
| Procedure | CPT List | |||||
| Hysterectomies | 58150 | 58152 | 58180 | 58200 | 58260 | 58262 |
| 58263 | 58267 | 58270 | 58275 | 58280 | 58285 | |
| 58290 | 58291 | 58292 | 58293 | 58294 | 58541 | |
| 58542 | 58543 | 58544 | 58550 | 58552 | 58553 | |
| 58554 | 58570 | 58571 | 58572 | 58573 | ||
| Robot Identification Codes | ||||||
| Type of Code | Code List | |||||
| ICD-9 | 17.41 | 17.42 | 17.43 | 17.44 | 17.45 | 17.49 |
| ICD-10 | 8E090CZ | 8E020CZ | 8E0X0CZ | 8E0Y0CZ | 8E0W4CZ | 8E093CZ |
| 8E0W3CZ | 8E0X3CZ | 8E0Y3CZ | 8E094CZ | 8E098CZ | 8E0W8CZ | |
| 8E0X4CZ | 8E0Y4CZ | 8E0W4CZ | 8E097CZ | 8E09XCZ | 8E0W7CZ | |
| 8E0WXCZ | 8E0XXCZ | 8E0YXCZ | ||||
| CPT | S2900 | |||||
Procedures were further classified as robot assisted or non-robotic based on the presence of specific ICD-9, ICD-10, or CPT codes within the procedure dates. The following codes were used for this distinction:The calculations for length of stay were based on the time between the first admission date and the last discharge date for inpatient procedures. Outpatient procedures were limited to events where the first date and last date difference was less than or equal to one. Prices were calculated at the individual DRG or CPT level as well as by bundling all ancillary services provided between the first and last dates as defined by the DRG or CPT codes. Nominal differences between robot assisted and non-robot assisted procedures were similar through both methodologies, and the numbers reported defaulted to the first methodology of prices at the individual DRG or CPT level.