
Half of American children have health insurance coverage through an employer (typically as a dependent on a parent’s coverage). Therefore, a major asset of employer-sponsored insurance (ESI) claims data is the opportunity to understand more about how children use and experience the health care system. In this brief, we use HCCI’s unique national dataset encompassing health care claims for over one-third of the population with ESI to explore one dimension of children’s health care use: hospital admissions.
Inpatient hospital admissions are a major component of health care use and spending. In this brief, we examine the reasons why children are admitted for inpatient care and whether and how these reasons differ from what sends adults to the hospital. We then assess whether the reasons children go to the hospital are different between general acute care hospitals and specialty children’s hospitals and how payments vary for services across these two types of hospitals. Finally, we examine how the first year of the COVID-19 pandemic affected children’s use of hospital services.
Over the 2016-2020 period, about 6% of the 25 million children in the HCCI data had an inpatient admission; this is similar to the percent of adults who had an inpatient admission in this period. Over 60% of the 1.6 million pediatric hospitalizations we observe from 2016-2020 were admissions of newborns and close to 40% of total pediatric inpatient spending was on newborn care. In this brief, we focus on non-newborn pediatric hospitalizations; these 698,000 hospitalizations were associated with $18.5 billion in allowed amounts and $647 million in patient out-of-pocket costs in the HCCI data in the 2016-2020 period.
We find that close to 30% of non-newborn pediatric admissions were for mental health needs. Other top causes for admission were for services associated with respiratory, digestive, and nervous system conditions. We also found that the vast majority—over 95%—of pediatric inpatient admissions were in general acute care hospitals. These hospitals provided more mental health services than children’s hospitals, where circulatory, nervous system, and other specialty care made up the majority of admissions. At the service level, payments were relatively comparable between general acute care and children’s hospitals; by category of admissions, average payment in children’s hospitals was higher, suggesting a more complex mix of services provided in those hospitals compared to general hospitals. Consistent with overall national trends, there was a decline in children’s inpatient admissions in 2020, the first year of the COVID-19 pandemic.
A child’s hospital admission can be a major event in a family’s life. Hospital care may be lifesaving, but also emotionally and financially burdensome. Understanding how children use these services is an important dimension of research that strives to improve the knowledge base regarding and foundation for improving the ESI system.
Close to 30% of Non-Newborn Children’s Hospitalizations were for Mental Health Services
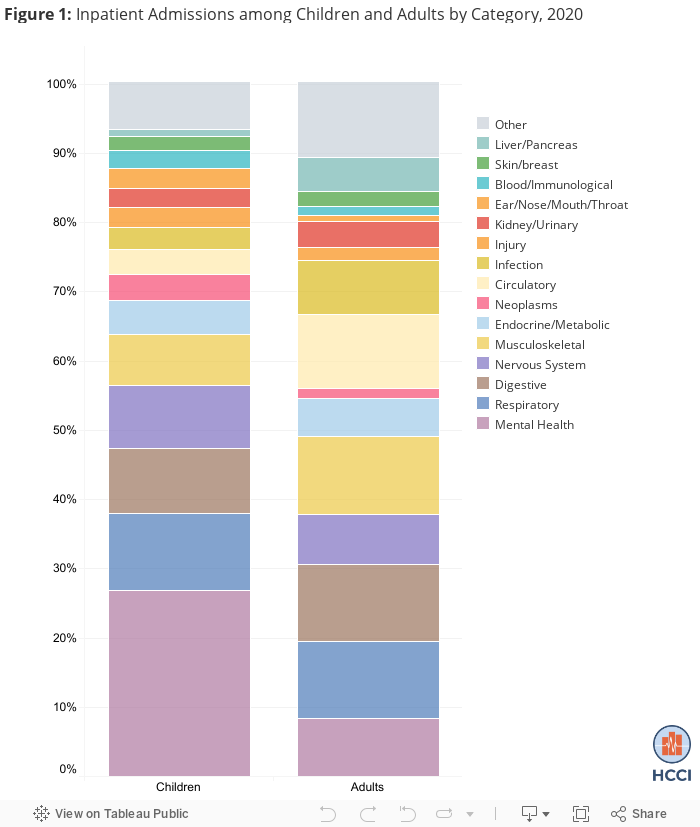
Just over 8% of non-newborn, non-childbirth hospital use was among children in 2020. The leading causes of non-newborn hospital admissions among children in 2020 were for services related to mental health (27%), respiratory conditions (11%), digestive conditions (10%), and nervous system conditions (9%).
As shown in Figure 1, the percent of admissions for mental health needs was substantially higher among children (27%) compared to adults (8%). Children had a lower percentage of admissions than adults for circulatory services (4% among children compared to 11% among adults) and infection (3% compared to 8%), but a similar percent of admissions for digestive, nervous system, and respiratory services.
(These data are available as downloadable data associated with HCCI’s 2020 Health Care Cost and Utilization Report. Note that results in this section may differ slightly from the rest of the brief as the analyses below were performed specifically for this brief and may differ slightly in methodology and sample.)
General Acute Care Hospitals Provide the Majority of Pediatric Inpatient Care, Including More Mental Health Care, Compared to Children’s Hospitals
The vast majority of pediatric inpatient care occurs in general acute care (GAC) hospitals. Consistently over 2016-2020, close to 90% of total pediatric inpatient spending and 95% of pediatric admissions occurred in GAC hospitals. In contrast to GAC hospitals, where nearly two-thirds of pediatric admissions were for newborn care, only 15% of admissions in children’s hospitals were newborns.
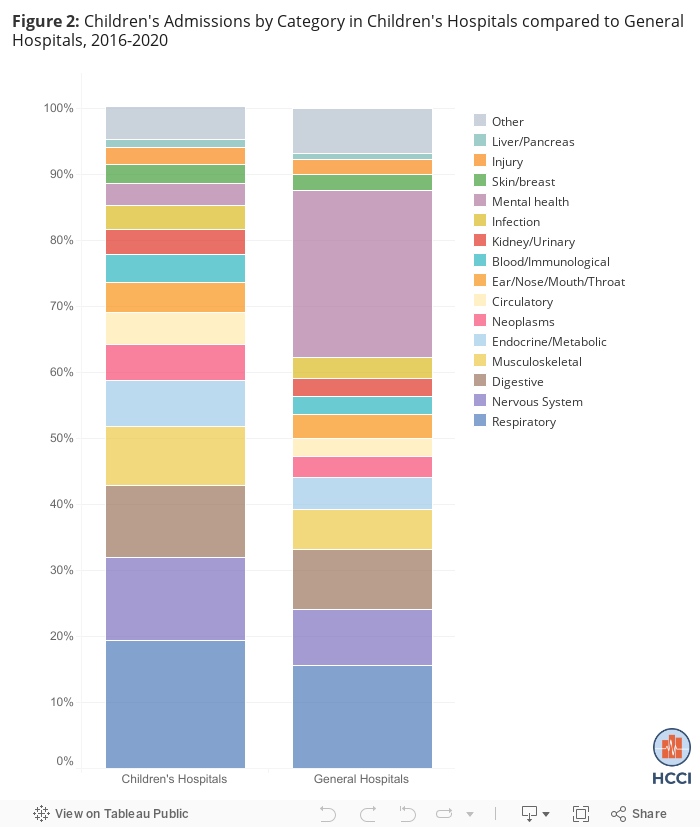
Among non-newborn admissions, a greater proportion of pediatric admissions in GAC hospitals were for mental health care needs (25%) compared to 3% of admissions in children’s hospitals (Figure 2). A greater proportion of admissions in children’s hospitals were for system-based specialty care such as nervous system services (13% of children’s hospital admissions compared to 8% of pediatric admissions in GAC hospitals), musculoskeletal services (9% compared to 6%), and cancer care (neoplasms; 5% compared to 3%).
Allowed Amounts were Higher at Children’s Hospitals than General Acute Care Hospitals, Likely Reflecting a More Complex Mix of Services
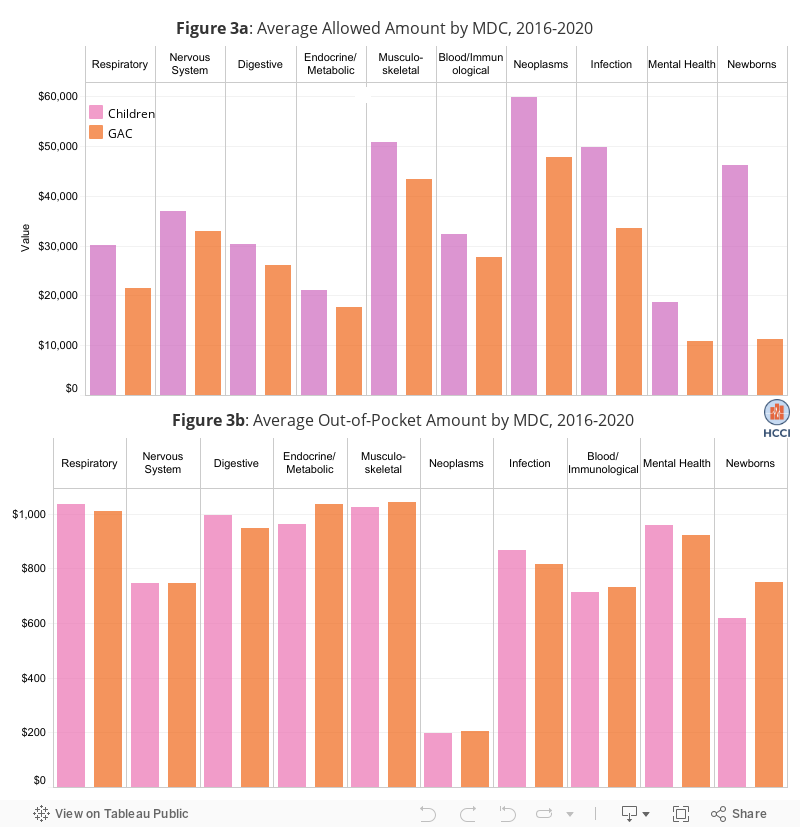
Across major diagnostic categories (MDCs), average allowed amounts (i.e., the amount paid by the health plan plus the amount paid by the patient) were higher at children’s hospitals than GAC hospitals (Figure 3a). For example, the average allowed amount for a mental health-related admission at children’s hospitals was $18,757 compared to $10,844 at GAC hospitals. The average allowed amount for an infection-related admission was $49,836 at children’s hospitals compared to $33,554 at GAC hospitals. Though total allowed amounts were generally higher at children’s hospitals than at GAC hospitals, the average amounts paid by patients were relatively similar (Figure 3b). For example, the average out-of-pocket payment for a respiratory admission was just over $1,000 in both children’s and GAC hospitals.
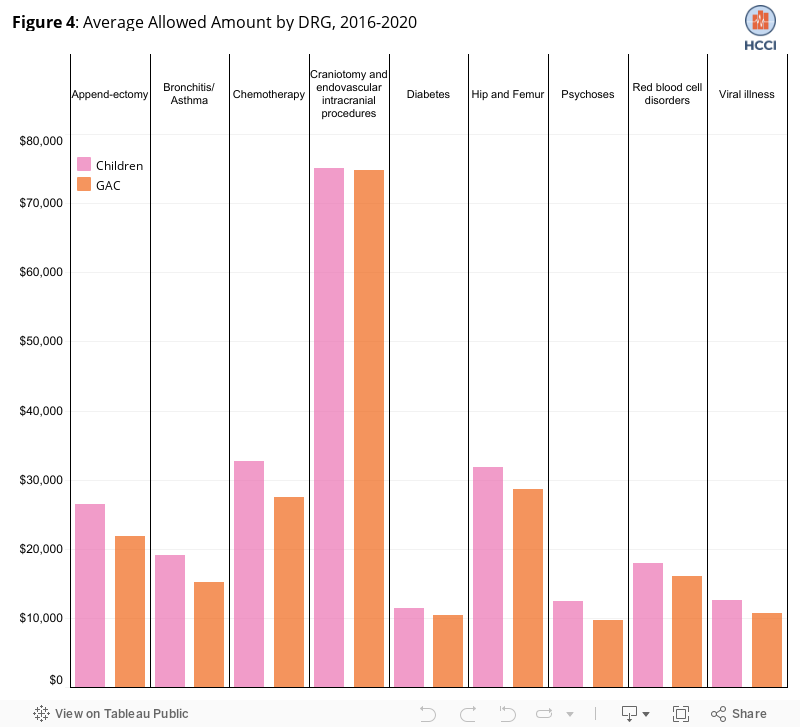
Higher health plan payments in children’s hospitals may reflect higher-reimbursed, more complex services due to the types of patients who are referred to these specialty hospitals as well as higher prices for the same services when provided in a children’s hospital than when the same service is provided in a GAC hospital. To explore how much of the variation in allowed amounts was due to different prices for the same services, we examined the highest-volume services (DRGs) within each MDC and found that allowed amounts were relatively similar between children’s and GAC hospitals at the DRG level (Figure 4). While this does not definitively answer the broader question about prices across hospital types, it suggests that the mix of services likely differs meaningfully across children’s and GAC hospitals and is related to spending differences.
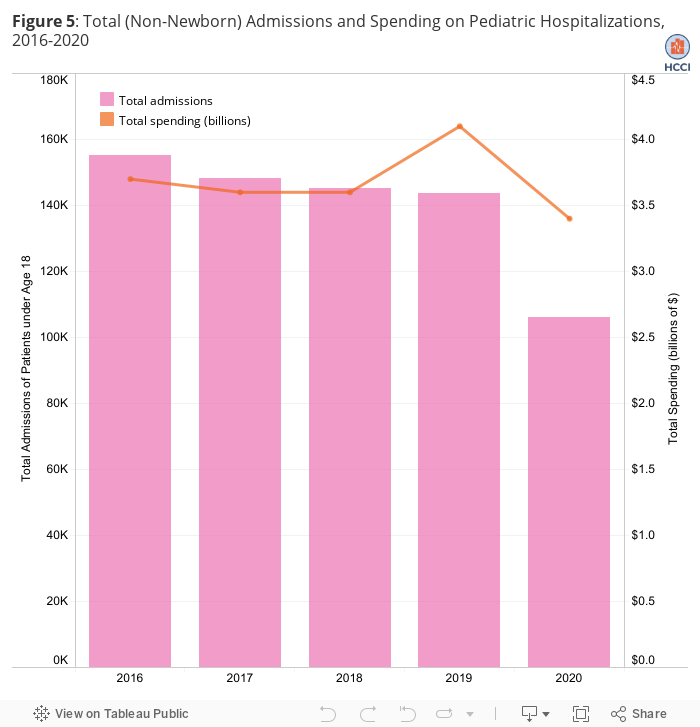
Children’s Hospital Admissions Declined in 2020, Particularly Early in the Year
Consistent with declining inpatient services in the broader population in the first year of the COVID-19 pandemic, we observed a substantial drop in the number of non-newborn pediatric inpatient admissions in our sample from 143,548 in 2019 to 105,916 in 2020. Also consistent with patterns in the full population, spending on pediatric hospitalizations increased due to rising prices even as volume fell over the 2016-2019 period, from $3.7 billion in 2016 to $4.1 billion in 2019. This increase was followed by a decline to $3.4 billion in 2020.
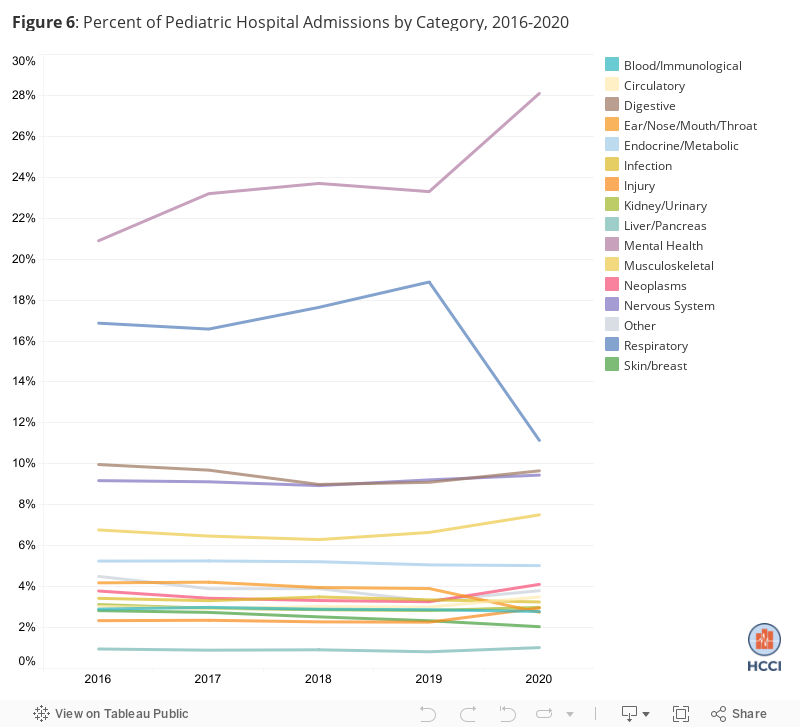
The percent of (non-newborn) admissions for mental health services increased from 23% to 28% from 2019-2020 while the percent for respiratory needs decreased from 19% to 11% (Figure 6). The decrease in respiratory admissions among children is likely due to a decline in common childhood respiratory illnesses (e.g., RSV) associated with masking in schools and schools being closed due to the pandemic in 2020. The percent of admissions made up by other categories of services has been largely consistent over time, including in 2020.
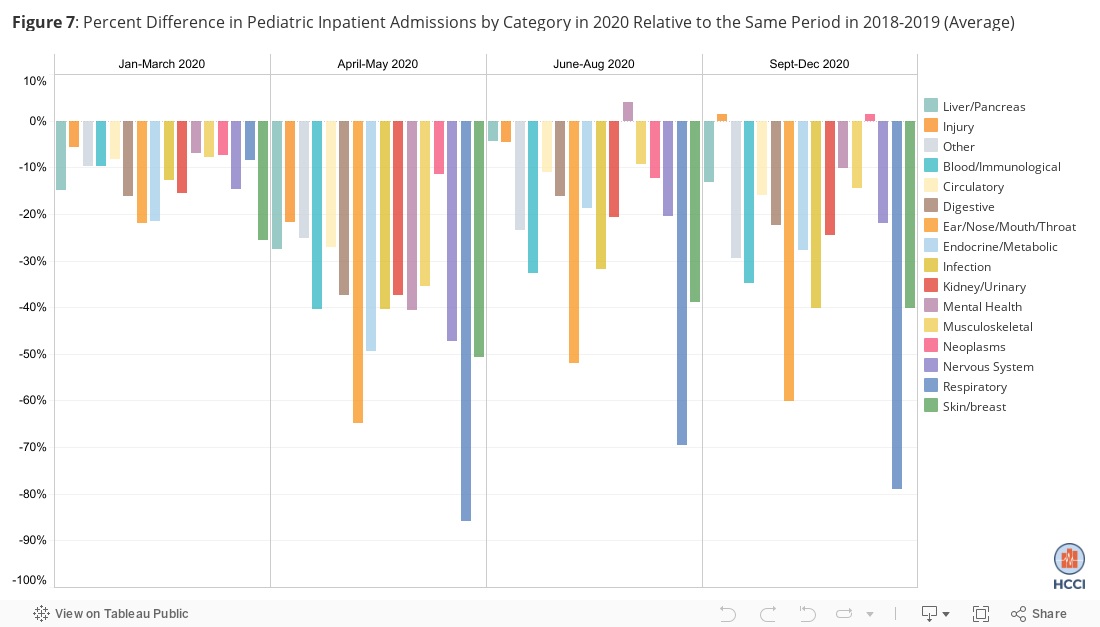
To examine the decline in pediatric inpatient admission volume in 2020 more closely, we compared use of services during different periods of 2020 to the analogous periods in 2018 and 2019 (combined). Consistent with other HCCI work on changes in service use and spending during the first year of the pandemic, we observed the most substantial declines in the volume of children’s hospital admissions in April-May of 2020. Some services remained lower than pre-pandemic levels throughout the end of the year while others rose (Figure 7).
We observed the largest declines in respiratory and ear/nose/throat admissions in April-May 2020 and throughout the end of the year. In April-May, we observed the smallest declines in cancer care and injury-related admissions; volume of these admissions also returned to pre-pandemic levels more quickly than other types of admissions.
High Rates of Mental Health-Related Admissions and Other Findings Point to Focus Areas in Efforts to Improve Children’s Health Care
A deeper understanding of why children are admitted to the hospital can help identify and target interventions to improve access to care and ultimately improve children’s well-being. Given that health in childhood has lasting effects into adulthood, these efforts can have compounding effects over time as well as impact children’s educational and other opportunities. For example, we find that close to 30% of children’s hospitalizations were for mental health needs. We do not explore here whether these hospitalizations are appropriate, and, in many cases, they may be necessary and even lifesaving. A high rate of inpatient mental health care, however, may also be a signal of inadequate preventive care and management of mental health needs in this population.
We also find, consistent with other evidence, that the majority of pediatric inpatient care is provided at general acute care hospitals. Thus, it is important for policymakers and hospital administrators to ensure that these hospitals have the necessary resources (e.g., staff) to meet children’s needs and that children’s health measures are included in general hospital quality metrics to incentivize care improvement.
This brief examines high-level characteristics of and trends in hospital admissions among children with ESI. We do not examine trends in hospital use among children with insurance through Medicaid, the other major source of coverage for this population. Evidence has shown that children living in communities characterized by high poverty levels and who are in racial and ethnic minority populations are disproportionately more likely to experience a hospitalization. Many children who are hospitalized have multiple chronic conditions, or other complex needs. Further evidence on how medical and social risk interact with children’s hospital use among children with ESI as well as those with Medicaid is needed as one component of efforts to ensure that the health care system meets the needs of all children.
Methods
Pediatric inpatient hospitalizations were identified between 2016 and 2020 using facility claims among enrollees with age band code that denotes age ranges between 0 and 17. We restricted our analysis to adjudicated inpatient claims with an employer-sponsored insurer health plan as the primary payer and allowed amounts greater than $1. While multiple Diagnosis-Related Group (DRG) codes may be assigned during an inpatient stay, we assigned the DRG with the highest allowed amount during the inpatient stay as the primary DRG for that stay. Inpatient hospitalizations were then classified by Major Diagnosis Condition (MDC) using the corresponding DRG assigned to the inpatient stay. The “other” category includes services assigned the following MDCs: Childbirth/Pregnancy, Health Status Factors, Female Reproductive, Male Reproductive, Trauma, Burns, Eye, Substance Use. We excluded the following inpatient admissions with the following MDCs from our analysis due to small sample sizes: Pre-MDC, HIV, ungroupable, hospice, skilled nursing facilities, and home health. We identified children’s hospitals using data from the National Plan and Provider Enumeration System.