The onset of the COVID-19 pandemic fundamentally shifted health and health care in the US in 2020. Hospitals have been central to responding to the pandemic and treating COVID, which means that hospitalizations can provide an important lens to understanding the pandemic’s impact. Earlier HCCI research looked at hospital use and spending among people with employer-sponsored insurance (ESI) before the pandemic to provide a point of comparison and the 2020 Health Care Cost and Utilization Report describes how spending changed across health care, including hospitals.
In this brief, we use Medicare and Medicaid claims data in addition to HCCI’s ESI claims dataset to examine COVID-related hospitalizations in 2020. We identified hospitalizations due to respiratory infections and inflammations, including COVID-19, in inpatient claims among all enrollees 18 years of age and older across ESI, Medicaid, and Medicare. Hospitalizations are reported as a rate per 100,000 enrollees to compare results across populations.
As expected, we find that 2020 hospitalization rates were highest among Medicare beneficiaries, the majority of whom are age 65 and older. Across ESI, Medicaid, and Medicare enrollees, the rate of hospitalizations was highest among people who live in more socially vulnerable areas and among American Indian and Alaskan Native, Black, and Hispanic enrollees.
Across Payers, COVID-related Hospitalizations Peaked in December 2020
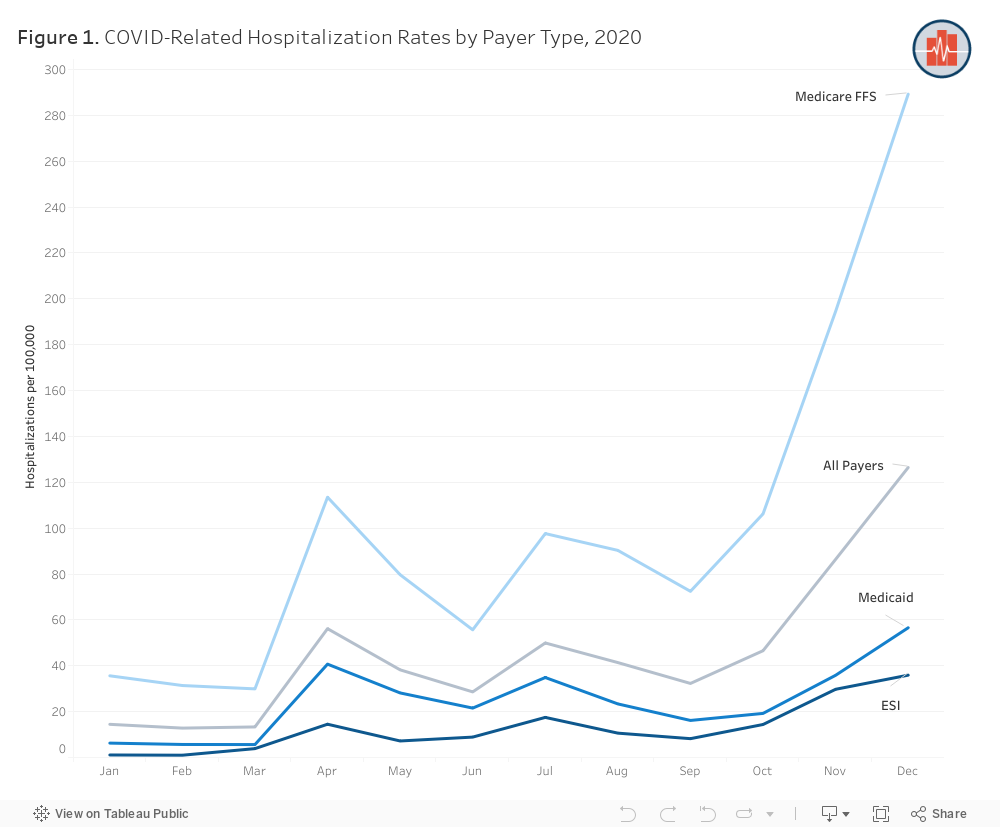
Figure 1 shows hospitalization rates by payer and month. In keeping with the trajectory of the pandemic, COVID-related hospitalizations were relatively rare in the first three months of 2020, with an average monthly rate of 14 hospitalizations per 100,000 enrollees among all payers combined. Beginning in March 2020, coinciding with the declaration of COVID-19 as national emergency, hospitalization rates increased considerably. There were spikes in hospitalizations in April and July 2020, but these were eclipsed by the hospitalization rate in December 2020, which reached an average of 126 per 100,000 enrollees, an increase of nearly 800% compared to March 2020.
Medicare Beneficiaries had the Highest Rates of COVID-19 Hospitalization
The COVID-related hospitalization rate was highest among the Medicare population, followed by Medicaid, and lowest among the ESI population (Figure 1). In December, the hospitalization rate among the Medicare population was nearly 290 per 100,000 enrollees. That rate was over five times higher than the Medicaid rate of 57 hospitalizations per 100,000 and over eight times higher than the ESI rate of 36 hospitalizations per 100,000 in that month.
The higher rate of COVID-related hospitalizations among Medicare enrollees reflects the fact that older adults are far more likely to be hospitalized due to the disease. Across all three payers, the rate of COVID-related hospitalizations during 2020 was higher among older enrollees; in ESI, for example, people aged 55-64 were almost six times more likely to be hospitalized than those aged 25-34 (319 hospitalizations per 100,000 enrollees compared to 47).
Hospitalizations were Highest among People Living in More Vulnerable Areas
Existing evidence shows that the pandemic has highlighted and exacerbated health disparities faced by vulnerable communities in the U.S. To examine these disparities in the context of COVID-19 related hospitalization, we linked our claims data with data from the Centers for Disease Control and Prevention’s Minority Health Social Vulnerability Index (MH-SVI), developed by the Office of Minority Health and the Centers for Disease Control and Prevention. MH-SVI measures the social determinants of health that make a community more or less vulnerable before, during, and after public health emergencies. The index is a composite measure of factors that include socioeconomic status, household composition and disability, minority status and language, housing type and transportation, health care access and infrastructure, and medical vulnerability.
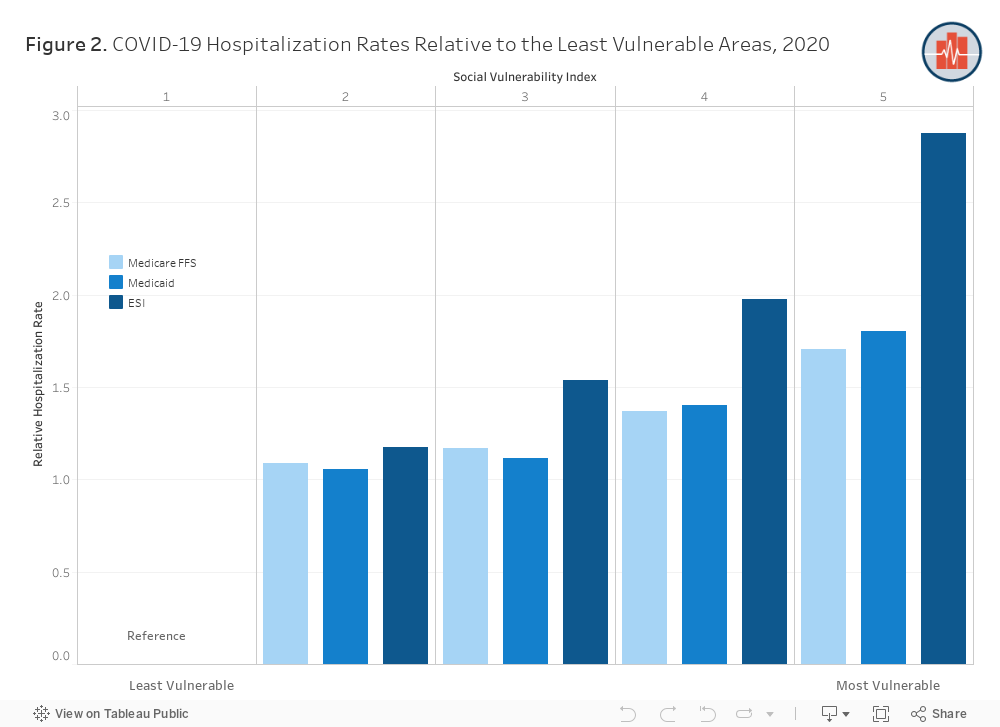
We find that more vulnerable communities experienced higher rates of COVID-19-related hospitalization. Figure 2 compares the COVID-related hospitalization rate for each SVI quintile to the least vulnerable quintile. For example, among the Medicaid and Medicare populations, the hospitalization rate was about twice as high among people living in the most socially vulnerable areas (SVI quintile 5) compared to those in the least socially vulnerable areas (SVI quintile 1), or 1524 hospitalizations per 100,000 enrollees compared to 893 hospitalizations per 100,000 enrollees for Medicare population, and 364 hospitalizations per 100,000 enrollees compared to 201 hospitalizations per 100,000 enrollees for Medicaid population. Among people enrolled in ESI, the hospitalization rate in the most vulnerable areas was almost three times higher than the rate among ESI enrollees residing in the least vulnerable areas (240 hospitalizations per 100,000 compared to 83). Compared to the Medicare and Medicaid populations, COVID hospitalizations increase at a faster rate among ESI enrollees with every increase in SVI quintile. More work is needed to better understand the factors that contribute to this rate disparity.
American Indian and Alaska Native Populations Experienced Disproportionately High Rates of COVID-19 Hospitalization
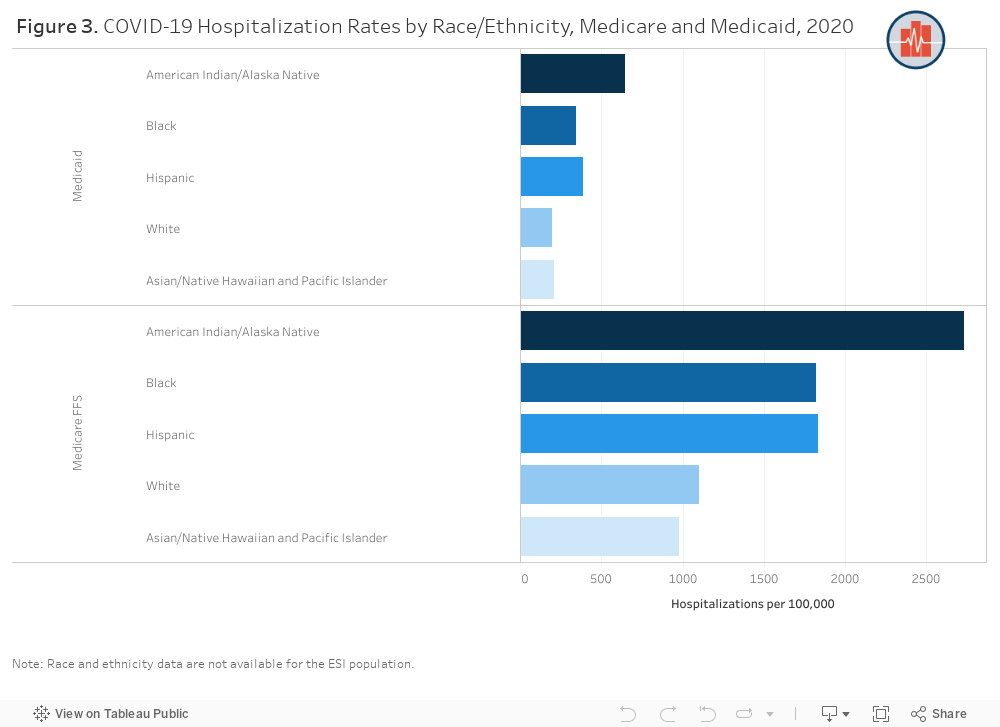
Figure 3 shows the annual COVID-related hospitalization rate by race and ethnicity among the Medicare and Medicaid populations (race and ethnicity data are not available in the ESI data). Within both populations, hospitalization rates were highest among American Indian or Alaska Native people, followed by Hispanic people and non-Hispanic Black people, and lowest for non-Hispanic white people and Asian or Pacific Islander people.
For example, in Medicaid, the rate of hospitalization was over three times higher among American Indian or Alaska Native people than among non-Hispanic white people (the population with the lowest hospitalization rate). In Medicare, the rate among the American Indian or Alaska Native population was 2.8 higher than the Asian or Pacific Islander populations. Among both Medicare and Medicaid enrollees, the hospitalization rates for Hispanic and non-Hispanic Black people were almost twice as high as rates among non-Hispanic white people. These results are consistent with other evidence that people of color are at increased risk of exposure to COVID-19 and experience higher rates of chronic medical conditions associated with more severe cases of COVID-19.
When Medicare and Medicaid data are combined without any age adjustment, we see a higher rate of hospitalizations among non-Hispanic white people compared to Hispanic people (not shown here). This reflects the higher rate of hospitalization among Medicare beneficiaries, who make up over two-thirds of the combined population, and who are older and predominantly white compared to Medicaid enrollees. This finding is consistent with other work and highlights the importance of adjusting for age when combining these payer types given that hospitalization risk is related to age, and age distribution differs by payer type.
Data Show where Inequality and Disease Burden Meet and Where More Resources Are Needed
The COVID-19 pandemic has affected the health and livelihoods of Americans in unprecedented ways. Among patients with COVID‐19, the risk of severe illness increases with age and is high among people with underlying conditions, such as a weakened immune systems, obesity, diabetes, and hypertension. Furthermore, people of color have been shown to have an increased risk of hospitalization and death due to COVID‐19. Our findings regarding COVID-19 hospitalizations among people with ESI, Medicare, and Medicaid underscore the disparate impact of the pandemic by insurance type, social vulnerability, and race and ethnicity.
One limitation of these findings is that they only contain data from 2020; continued monitoring of COVID-19 hospitalizations as additional years of data become available is critical, especially as new variants, vaccinations campaigns and other clinical intervention strategies alter who is affected most by COVID-19.
Ongoing monitoring of hospitalization rates is essential in efforts to strengthen public health prevention strategies. Understanding the differential impact of health emergencies by social vulnerability and race should help policymakers prioritize equitable resource allocation. Our findings highlight the importance of providing equitable access to preventive measures, such as COVID-19 vaccines, to protect those who need the support the most. These and other efforts to address structural and societal factors that impact health care access and outcomes are critical for future global crises.
Methods Note
The COVID-19 hospitalization (DRG 177-179) rates were calculated as the total number of COVID-19 inpatient admissions amongst the population divided by the total population per 100,000 enrollees. The DRG codes used in this analysis are as follows:
- DRG 177 – Respiratory Infections & Inflammations w/MCC
- DRG 178 – Respiratory Infections & Inflammations w/CC
- DRG 179 – Respiratory Infections & Inflammations w/o CC/MCC
Data are available at a monthly level for each payer in the downloadable data. The analysis above includes results for combined analysis at the year level for 2020.
Our results show the crude rates, we did not adjust by age.
All datasets were restricted to beneficiaries greater than or equal to 18 years of age.
For our ESI analysis, we are required to have at least 100 admissions per demographic being reported. Therefore, data may be missing in some categories.
We included claims from the Medicare Fee-for-Service (FFS) dataset and the Medicaid dataset. The Medicare FFS dataset was restricted to beneficiaries fully enrolled in Medicare FFS Part A and Part B, including Medicaid dual enrollees.
The Medicaid dataset excluded those who were dual enrolled in Medicare (to avoid double counting dual-enrolled beneficiaries), as well as those with missing eligibility information or restricted benefits.
Additionally, the following states were excluded from the Medicaid dataset due to poor data quality: Alabama, Kansas, and Tennessee. All datasets were restricted to beneficiaries with known age and sex, as well as those who lived in the United States. Medicaid race and ethnicity data were restricted to states with reliable data on race and ethnicity.