
The federal 340B Drug Discount Program was created in 1992 to lower the cost of drugs for non-profit hospitals that disproportionately care for people with lower incomes. Under the program, discounts from drug manufacturers to hospitals are estimated to range from 20 to 50% on most outpatient medications, although the actual discounts are not publicly disclosed.
Because the program does not restrict the patients who can receive drugs purchased through the 340B program, they can be administered to patients of all income levels with any type of insurance, including employer-sponsored insurance and Medicare. The lower acquisition costs do not seem to lead to a corresponding decrease in payments. Thus, increasing the potential margin hospitals can earn from administered drugs.
Several studies have suggested that the 340B Program’s financial incentives may be leading to unintended consequences. For example, in areas with a 340B hospital, enrollees in Traditional Medicare were more likely to receive their cancer drugs in an outpatient department than a physician office than in areas with no 340B hospital. Other research found that, following a hospital’s initial participation in the 340B program, oncology drug spending increased among people with employer-sponsored insurance. At the same time, evidence has been mixed on whether 340B participation is associated with community benefits, such as uncompensated or charitable care. Since 2000, the number of registered 340B entities grew from 8,100 to over 50,000, primarily driven by hospital-based 340B participation.
This report assesses whether a hospital’s participation in the 340B program is associated with different patterns of use (including shifts in site of care), prices, and out-of-pocket spending on common administered drugs used by people with blood cancers and autoimmune diseases between 2018 and 2022 among people with employer-sponsored insurance, Medicare fee-for service, and Medicare Advantage (See Methods). Outcomes in this report contain only the use and price of therapeutic drug agents and do not include fees for drug administration and other ancillary services.
From 2018 to 2022, we observe an increase in the proportion of drug administration provided in hospital outpatient departments overall and a decrease in the proportion provided in physician offices. That pattern was particularly pronounced among 340B participating hospitals. 340B hospitals were also associated with higher employer-sponsored insurance prices than non-340B hospitals. We found out-of-pocket amounts paid by ESI enrollees were lower across all three sites of care (i.e., 340B hospital outpatient department, non-340B hospital outpatient department, and physicians’ office) compared to Medicare FFS. Out-of-pocket amounts among blood-cancer related oncology drug administrations grew faster than among autoimmune disease-related drug administrations in ESI and Medicare FFS and across all sites of care.
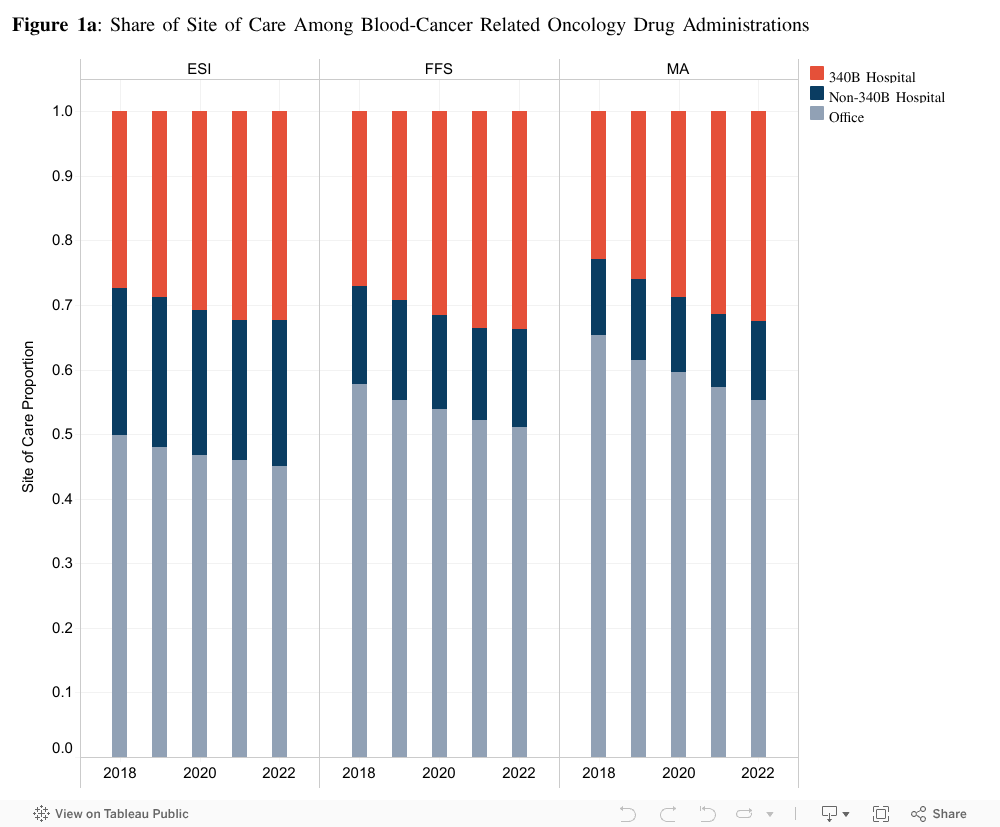
Physician-administered drugs have shifted from physician offices to outpatient departments, at faster rate for 340B hospitals
Overall, the share of blood-cancer related oncology drug administrations rendered at any hospital outpatient department grew 9% between 2018 and 2022 (Figure 1a). As shown in Figure 1a, growth over that period was faster among 340B hospitals than non-340B hospitals. Among people with ESI, the share of blood-cancer oncology drug administrations that took place in a 340B hospital outpatient department grew from 27% in 2018 to 32% in 2022 (an 18% increase). The share that took place in a non-340B hospital outpatient department stayed at 23% over the same period while drug administrations that took place in a physician’s office decreased from 49% to 45% (a 10% decrease).
From 2018 to 2022, the proportion of blood-cancer related oncology drug administrations among Medicare FFS provided at 340B hospitals went from 27% to 33%. The proportion provided at non-340B hospitals remained flat at approximately 15%, and the proportion provided at physician offices decreased from 57% to 51%. A similar pattern was observed in Medicare Advantage.
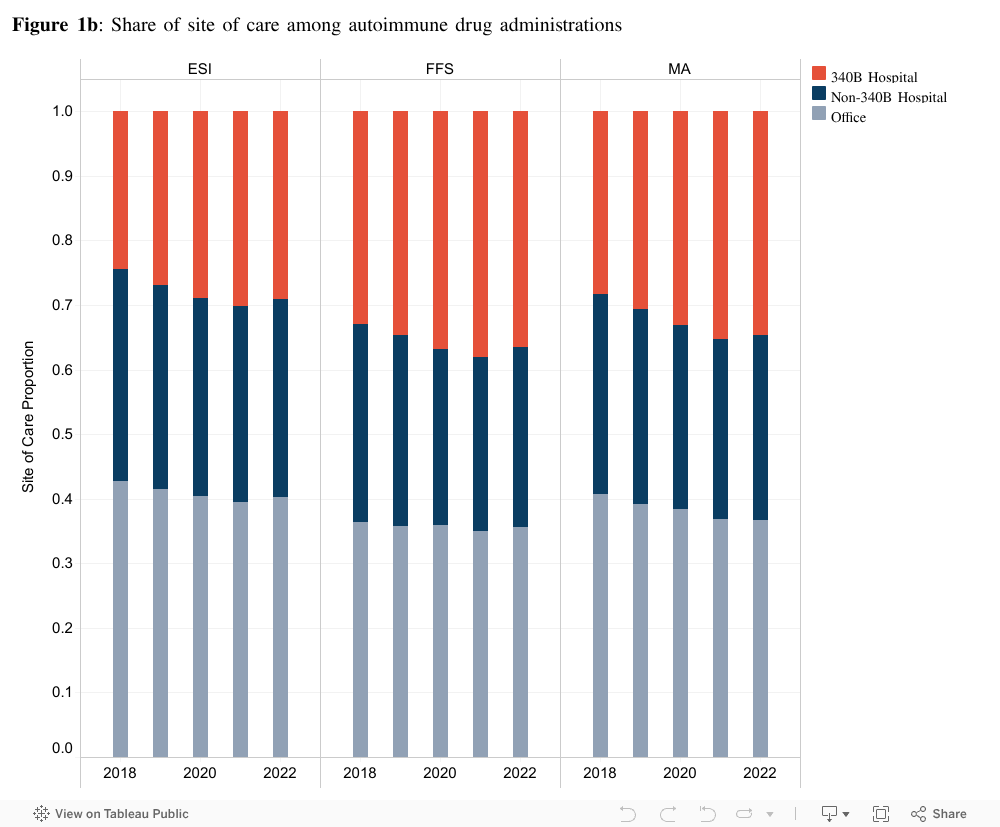
Among autoimmune disease administered drugs, we observed a similar but less dramatic pattern of site of care trends (Figure 1b). The share of autoimmune administrations in ESI provided in any hospital outpatient department grew by 8% from 2018 to 2022. Similar to blood-cancer related oncology drug administrations, we found that the share of drug administrations in 340B-affiliated hospital outpatient departments increased between 2018 and 2022 while administrations at non-340B hospital outpatient departments and physician’s offices decreased.
From 2018 to 2022, among people with ESI, the share of autoimmune drug administrations that took place in a 340B hospital outpatient department grew from 24% to 29% (a 21% increase). At the same time, the share of autoimmune drug administrations that took place in a non-340B hospital outpatient department decreased from 32% to 30% (a 6% decrease). The share that took place in a physician’s office decreased from 42% to 40% (a 5% decrease).
A similar pattern was observed in Medicare FFS and Medicare Advantage. Among people with Medicare FFS, the share of autoimmune drug administrations that took place in a 340B hospital increased from 33% to 37% (12%) from 2018 to 2022. At the same time, the share of autoimmune drug administrations that took place in a non-340B outpatient department decreased from 31% to 28% (a 10% decrease), and the share in a physician’s office stayed constant at 36%.
Among people with Medicare Advantage, the share of autoimmune drug administrations that took place in a 340B hospital increased from 28% to 34% (a 21% increase). Those that took place in a non-340B hospital decreased from 31% to 29% (a 6% decrease). Drug administrations that took place in a physician’s office decreased from 41% to 37% (a 10% decrease).
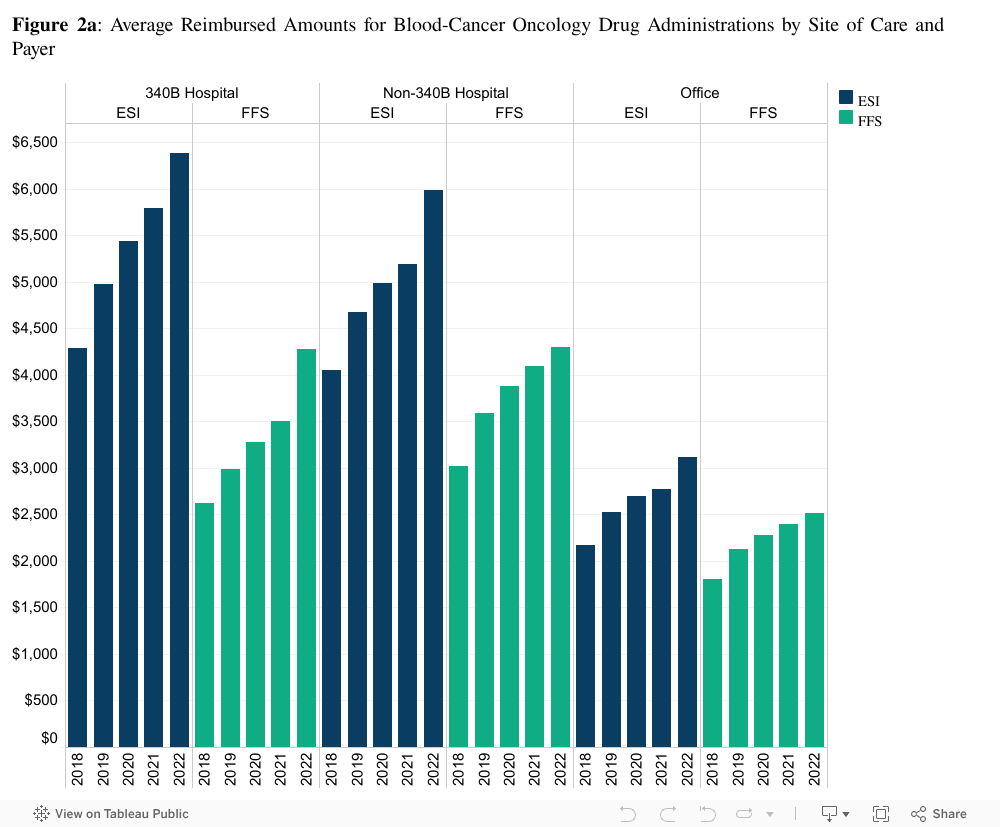
340B-affiliated hospitals received higher reimbursement rates among people with ESI
As shown in Figure 2a, 340B hospital outpatient departments had the highest average prices for blood-cancer related oncology drug administrations for employer-sponsored insurance. Among people with ESI, the average reimbursed amount in 2022 was $6,387 at 340B-affiliated hospital outpatient departments compared to $5,989 at non-340B hospitals outpatient departments, and $3,117 at physician offices.
Unlike employer-sponsored insurance, the 2022 Medicare fee-for-service average reimbursed amount was similar at 340B ($4,273) and non-340B ($4,303) hospitals. Both were substantially higher than reimbursement at physician offices ($3,518). This is because Medicare’s Hospital Outpatient Prospective Payment System (OPPS) reimburses 340B hospitals the same as non-340B hospitals.
In both ESI and Medicare FFS, reimbursement amounts for blood-cancer related oncology drug administrations grew the fastest at 340B-affiliated hospital outpatient departments. Specifically, average ESI payments increased by 49% in 340B hospitals, 47% in non-340B hospitals, and 43% in physician offices from 2018 to 2022. Similarly, Medicare payments grew 63% in 340B hospitals, 42% in non-340B hospitals, and 39% in physician offices. Differences in Medicare payment between 340B and non-340B hospitals can be attributed to case mix of oncology therapeutic drug agents (See Methods for limitations).
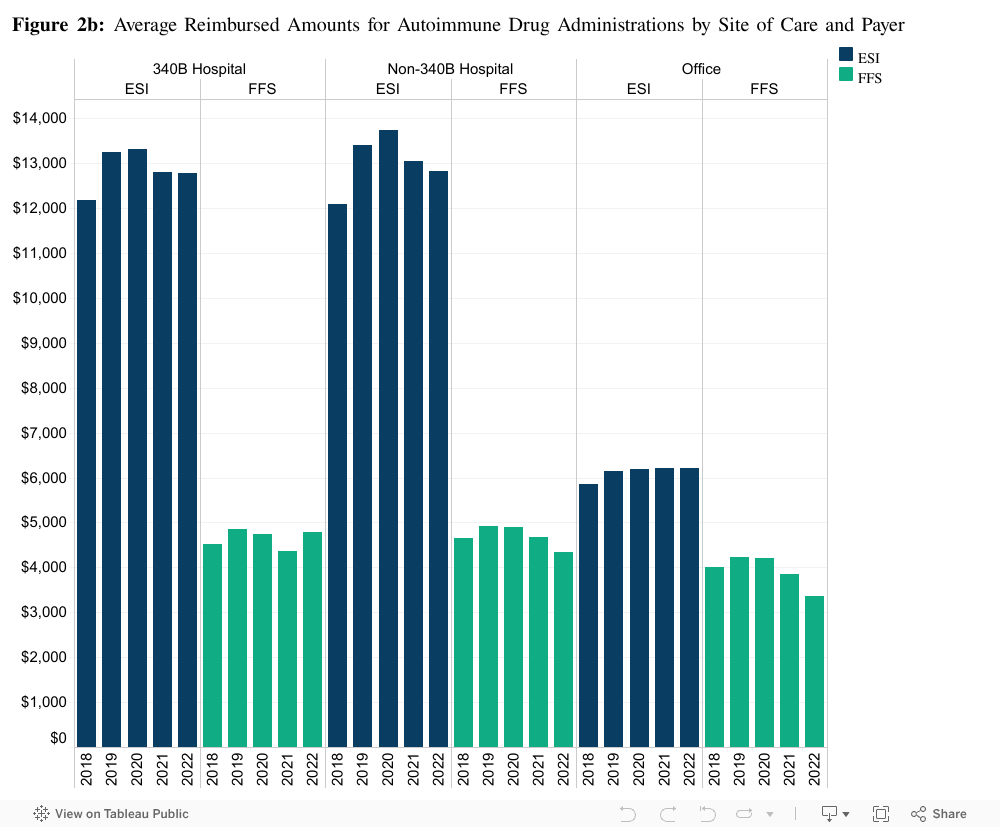
Average reimbursed amounts for autoimmune drug administrations were relatively similar between 340B and non-340B hospital outpatient departments and lowest among physician offices for in both ESI and Medicare FFS (Figure 2b). For example, the average ESI reimbursement amount for an autoimmune drug administration at a 340B hospital outpatient department in 2022 was $12,775 compared to $12,834 at a non-340B hospital and $6,221 at a physician’s office.
Medicare FFS reimbursement for autoimmune drug administrations at 340B hospitals also was similar to non-340B hospitals. The average reimbursement amount for an autoimmune drug administration at a 340B hospital outpatient department in 2022 was $4,798 compared to $4,338 at a non-340B hospital and $3,363 at a physician office.
Growth in the average ESI and Medicare FFS payment was less pronounced among autoimmune drug administrations than among the blood-cancer related oncology drug administrations. From 2018 to 2022, ESI payments grew 4% at 340B hospitals, 6% at non-340B hospitals, and 6% at physician offices. The introduction of biosimilar competitors since 2017 may have moderated the growth of the reimbursement amounts for autoimmune drugs.
Higher reimbursement to 340B hospitals can lead to higher out-of-pocket payments
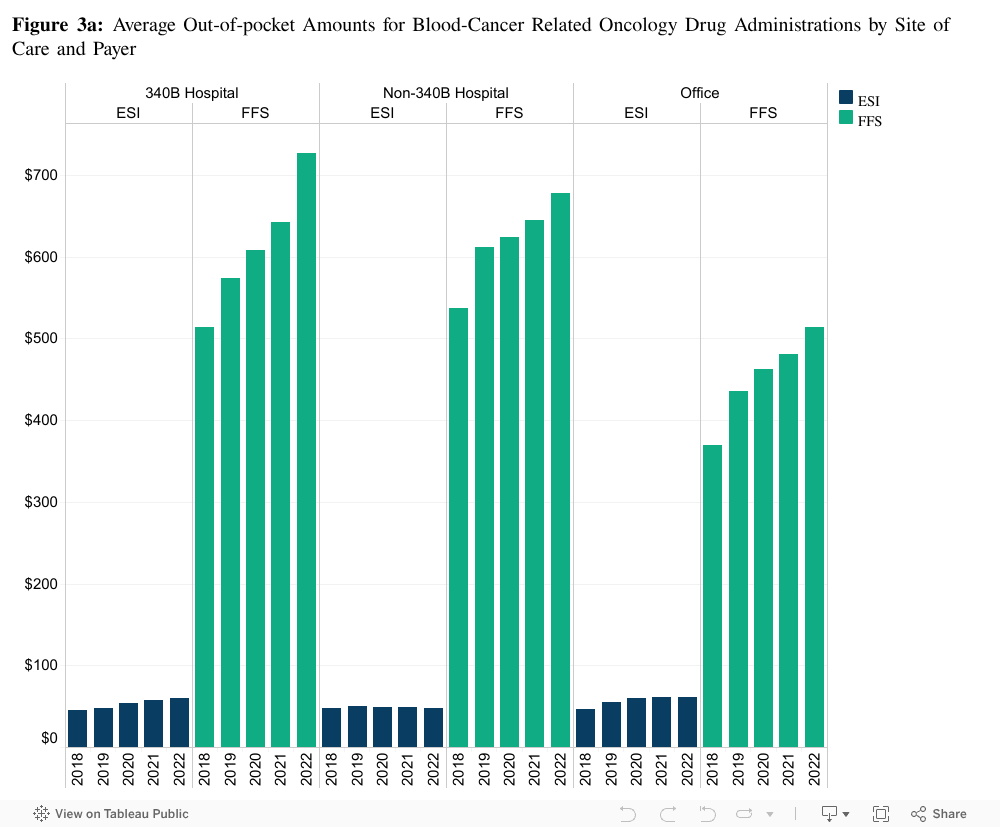
The observed differences and patterns in reimbursement rates among 340B hospitals, non-340B hospitals, and physician offices are also reflected in the out-of-pocket amounts paid by patients. Across both payers and types of administered drugs, we found that high average reimbursement amounts were associated with higher out-of-pocket amounts. In 2022, among people with ESI, the average out-of-pocket payment for a blood-cancer oncology drug administration at a 340B hospital was $59. The average out-of-pocket payment at a non-340B hospital was $48, and the average out-of-pocket payment at a physician’s office was $60 for an oncology drug administration in 2022.
Medicare FFS does not offer the annual out-of-pocket maximum included in ESI plans. Accordingly, Medicare FFS enrollees tend to have out-of-pocket payments substantially higher than people with ESI. Medigap plans, however, often cover out-of-pocket costs, so the amounts presented here do not necessarily represent what Medicare beneficiaries pay after their Medigap benefit is applied. If Medicare FFS enrollees were to pay the full out-of-pocket amount for blood-cancer related oncology drug administrations, the average payment would be $727 at 340B hospitals, $677 at non-340B hospitals, and $513 at physician’s offices in 2022 (Figure 3a).
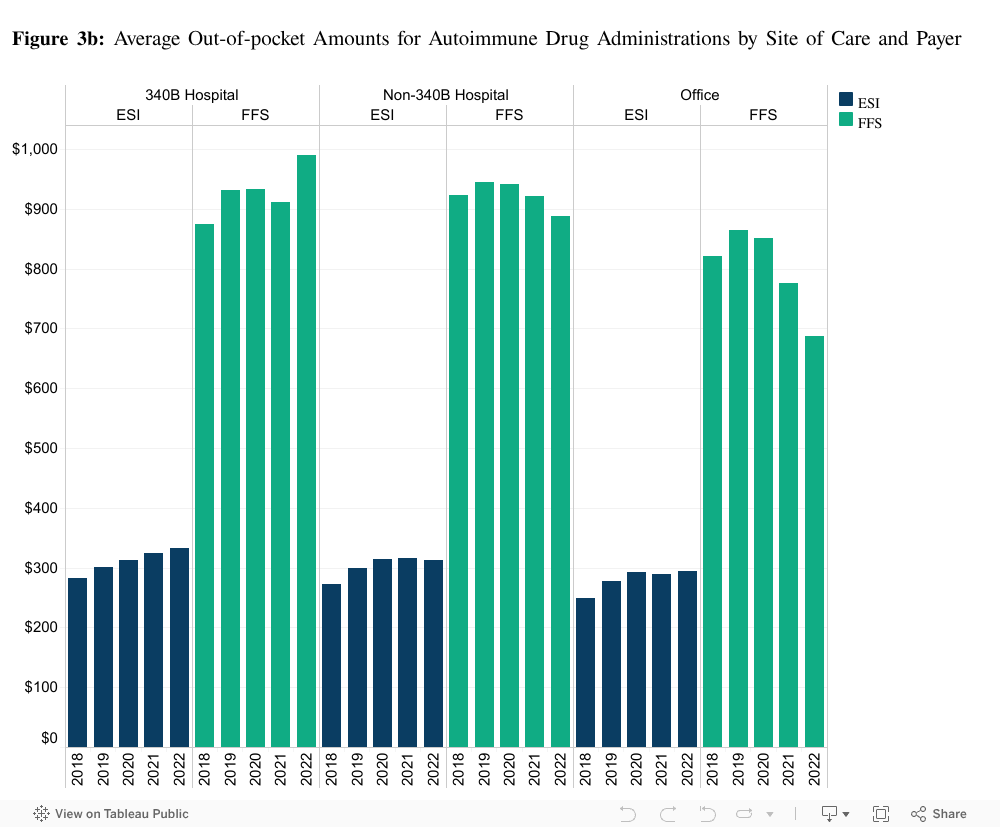
Among autoimmune drug administrations, average out-of-pocket amounts among people with ESI were higher at 340B hospitals. For example, in 2022, the average out-of-pocket payment was $332 at 340B hospitals, $313 at non-340B hospitals, and $294 at physician’s office. Average out-of-pocket amounts among people with Medicare FFS in 2022 were $991 at 340B hospitals, $887 at non-340B hospitals, and $687 at physician’s office. Differences in out-of-pocket amount by sites can be attributed to case mix or dosage (See Methods).
Impact of site-of-service shifts and 340B participation on patients
This report shows an increasing proportion of blood-cancer related oncology and autoimmune drugs are being administered in 340B hospital outpatient departments. This pattern was consistent among employer-sponsored insurance, Medicare fee-for-service, and Medicare Advantage.
Despite lower drug-acquisition costs, our analysis found that 340B hospitals received higher ESI payments that non-340B hospitals or physician offices for blood-cancer related oncology drugs. ESI payments for autoimmune drugs were similar between 340B and non-340B hospitals. As expected, Medicare reimbursement, which does not factor 340B participation into its payments, was similar between 340B and non-340B hospitals for blood-cancer related oncology and autoimmune drugs. The higher ESI payment, combined with discounts provided by the 340B program, mean that 340B hospitals generated more revenue than non-340B hospitals for the same drug administration.
In many instances, the higher payment amounts to 340B hospitals carry through to out-of-pocket costs borne by patients. In 2022, we found that out-of-pocket costs for patients receiving blood-cancer related oncology drugs from 340B hospitals were 23% higher than non-340B hospitals ($59 compared to $48). Among autoimmune drug administrations, patients pay 6% more at 340B outpatient departments than non-340B outpatient departments ($332 compared to $313). Generally, ESI benefit design includes limits on amounts individuals pay out-of-pocket for care, explaining why the gap in out-of-pocket costs is smaller than reimbursement.
This report also highlights that ESI and Medicare payments for drug administration are higher in hospital outpatient departments than in physician offices. This site differential payment also creates financial incentives for hospitals and health systems to acquire physician offices and to steer patients to outpatient departments for services that could be provided safely in either setting. (For a more detailed analysis of site of service differences, see this HCCI report.)
The growing share of drug administration at hospital outpatient departments, especially among 340B hospitals, is contributing to faster health care spending broadly. It also has a direct and growing impact on patients through cost sharing. Proposals such as site neutral payment, which reimburses providers at the same rate regardless of site of care, can address the out-of-pocket burdens and shift financial incentives away from greater concentration in outpatient services.
Persistently high health care costs, especially for patients requiring life-saving treatments, can force difficult decisions between health care and daily necessities (e.g., housing, food). These challenges are particularly acute among people with fixed incomes or people with lower incomes.
Acknowledgements
We would like to extend our appreciation to Blood Cancer United for their contributions to this project. Their expertise, insights, collaboration, and passion greatly enhanced the quality and depth of this project.
Methods
In this report, we used administrative claims data from Health Care Cost Institute, Medicare RIF, and Medicare Advantage Encounters data. We restricted our analysis to adjudicated outpatient facility and professional claims with the health plan as the primary payer and allowed amounts greater than $1 between 2018 and 2022. We identified administered drugs of interest using Healthcare Common Procedure Coding System (HCPCS) found in medical claims. Hospital outpatient departments affiliated with 340B hospitals were linked using Health Resources & Services Administration 340B registered entities database (downloaded March 2025) through provider encryption. The unit of analysis in this report is patient-service date for each administered drugs of interest.
Our analysis is accompanied by a few limitations. We do not directly control for case mix among the three sites of care, which can drive the underlying reimbursement amounts particularly among administrative pricing in Medicare fee-for-service. However, we limited our analyses to administered drugs among blood cancer patients to limit the noise introduced due to differential dosage for other cancers. A limitation in this report is that we examine the average reimbursed amount by ESI and Medicare fee-for-service, and does not take into account potential dosing differences by weight or starter/titration dosage in course of treatments. Our primary price outcome of interest is the average allowed amounts paid by the health plan to the provider. We did not identify whether clinics/practices were vertically integrated with 340B or non-340B health systems, therefore likely undercounting the prevalence of 340B program in all payer populations.