
Research has shown that the price of a single service provided in a hospital outpatient department is consistently higher than the same service provided in a physician office. An earlier HCCI analysis examined 46 services that could be provided in either setting and found higher prices in outpatient departments for all services in all years studied. More recently, we evaluated prices for laboratory tests in outpatient departments, independent laboratories, and physician offices. The median price for a lab test in an outpatient department was more than 3.5 times higher than the same test in an independent lab and 3.3 times higher than the same test performed in a physician’s office.
State and federal policymakers have considered and enacted a number of policies to address the difference in price associated with where a service is provided. With a goal of paying the same price for the same service no matter where the patient receives the care, one such policy option is establishing “site neutral” payments. Other policy options under consideration address higher prices in outpatient departments by regulating “facility fees.”
This brief explains what a facility fee is and illustrates one way they operate in practice. It then walks through two examples of the kinds of facility fees of greatest concern to consumers and policymakers.
Hospital care often results in two bills: one from a physician and one from the hospital.
When people receive care in a hospital, whether an inpatient admission (e.g. an overnight stay) or a health care service from an outpatient department, they frequently receive two bills. The first is for the costs associated with the care provided by physicians and other clinicians for their professional services. The second is for costs associated with care provided by the hospital, including room and board, procedures, and evaluation and management, with overhead costs (e.g., equipment, space, and support staff) included.
Technically, any amount billed by a hospital could be considered a facility fee. Policy efforts related to facility fees, however, can be targeted more narrowly. Generally, there is broad agreement that hospitals should be reimbursed for expenses incurred in providing care. Hospitals also may have higher expenses than physician offices, including those associated with licensing, accreditation, and regulatory requirements, and have overhead costs related to emergency room and other services the hospital must provide but that are not directly related to the care the patient received.
Most policy efforts related to facility fees have focused on care received outside of a hospital. If a physician’s office is owned by a hospital system, for example, a patient may be charged a facility fee in addition to the bill from the physician who provides care. In these cases, the physician’s office is allowed to bill as though the care was received in a hospital, despite no physical change in where patients are treated or the care they receive. As hospitals increasingly acquire physician practices, facility fees in these situations have become more common.
Identifying and quantifying facility fees can be challenging.
Better understanding the cost associated with facility fees and how frequently they are billed is a foundational step to determining whether and which policy intervention is necessary. In many instances, the facility fees of greatest policy interest are not easily identifiable in claims data, making it difficult to quantify their impact.
The analysis below uses primary care evaluation and management (E&M) office visits and pediatric wellness visits to illustrate an example of facility fees of concern to policymakers and to measure their financial impact. Using HCCI’s unique commercial claims dataset, which contains claims for more than 50 million Americans annually, we compared primary care and pediatric wellness visits in which only a physician billed for the service (“physician office”) and the same visits in which a physician and facility billed for the same code for the same patient on the same day (“outpatient setting”). We characterize the difference between those amounts as facility fees for purposes of the following analysis.
The estimated facility fee for adult primary care visits and pediatric wellness visits was approximately $100 in 2022.
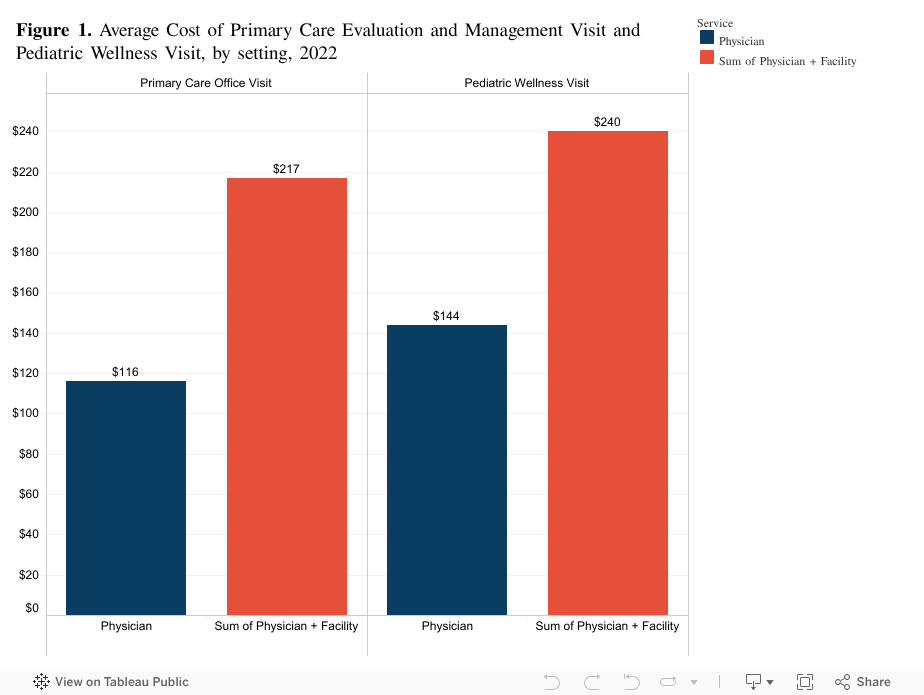
As shown in Figure 1, the average price for a primary care visit in a physician office was $116 in 2022. When the primary care visit takes place in an outpatient setting, the average price is 87% higher or $217. The $101 difference in price can be characterized as a facility fee and is the focus of many state and federal policy efforts.
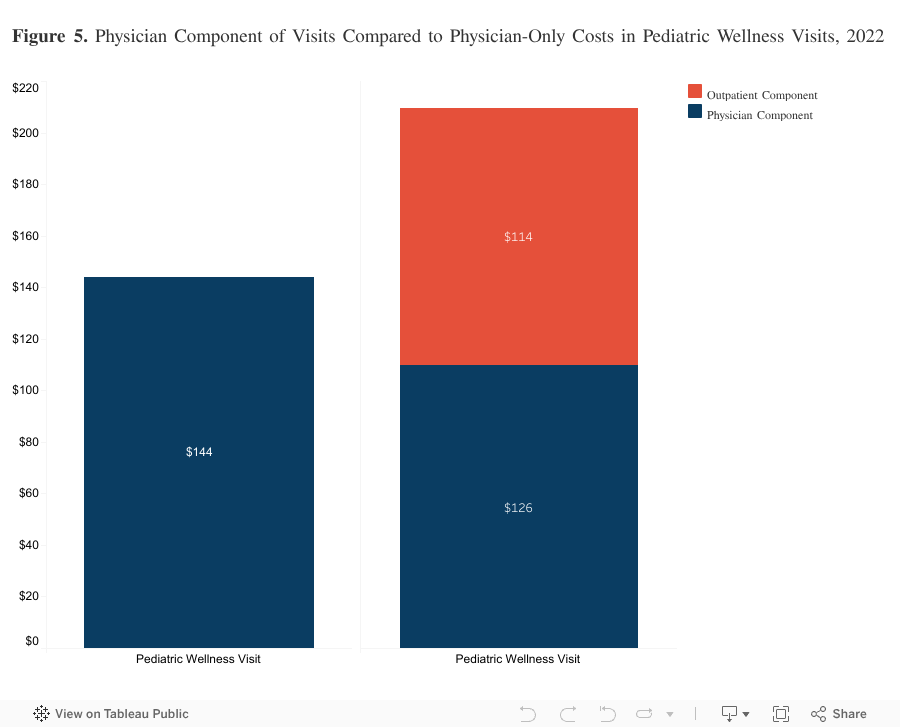
We see a similar difference between pediatric wellness visits provided in a physician’s office (average price of $144) and an outpatient setting ($240). The $96 (67%) price difference also would be considered a facility fee in this context.
Physician services make up roughly half of the cost of visits in an outpatient facility.
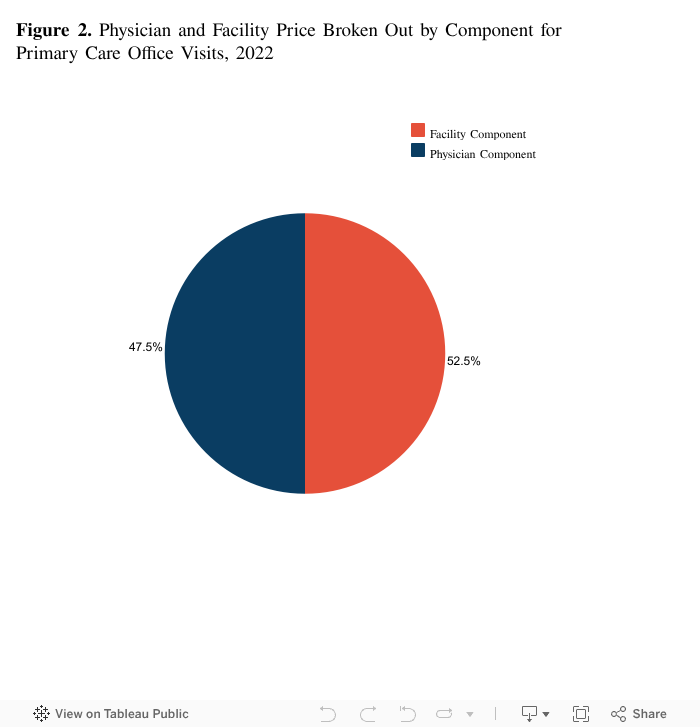
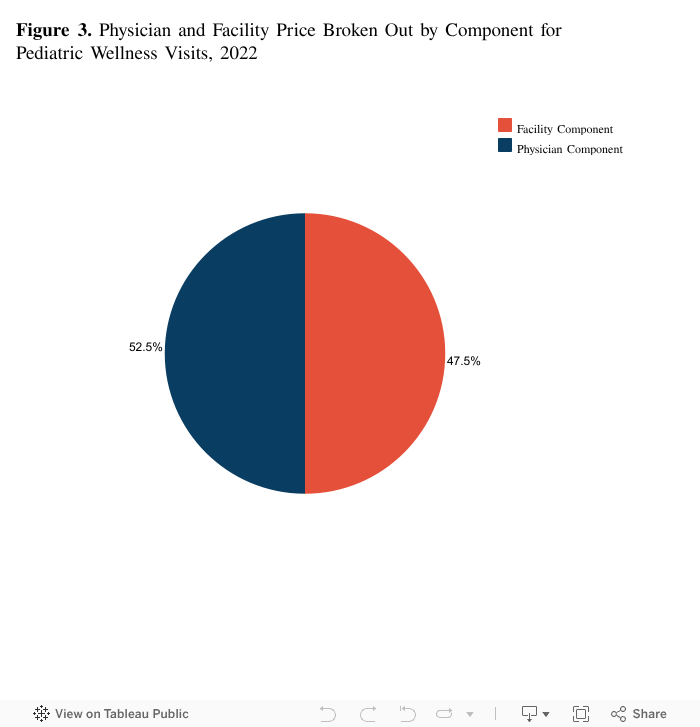
For those primary care visits that take place in an outpatient setting, the physician component of the prices made up a little less than half (47%) of the total cost. As illustrated in Figure 2, $103 of the $217 cost is for the physician component with the remaining $114 the outpatient facility fee. Pediatric wellness visits follow a similar pattern, though physician costs were slightly more than half of the total. Of the $240, $126 (53%) were for physician expenses with the remaining $114 going to the facility.
For both of these services, the physician-only costs of visits cover some administrative expenses. For visits in the outpatient setting, those overhead costs could appear either in the facility component or the physician component. Therefore, for this analysis, we estimate the facility fee as the difference between the outpatient total and the physician-only total (rather than the entire amount billed by the facility).
Physician costs associated with outpatient primary care visits are slightly lower, but facility fees dramatically offset the difference.
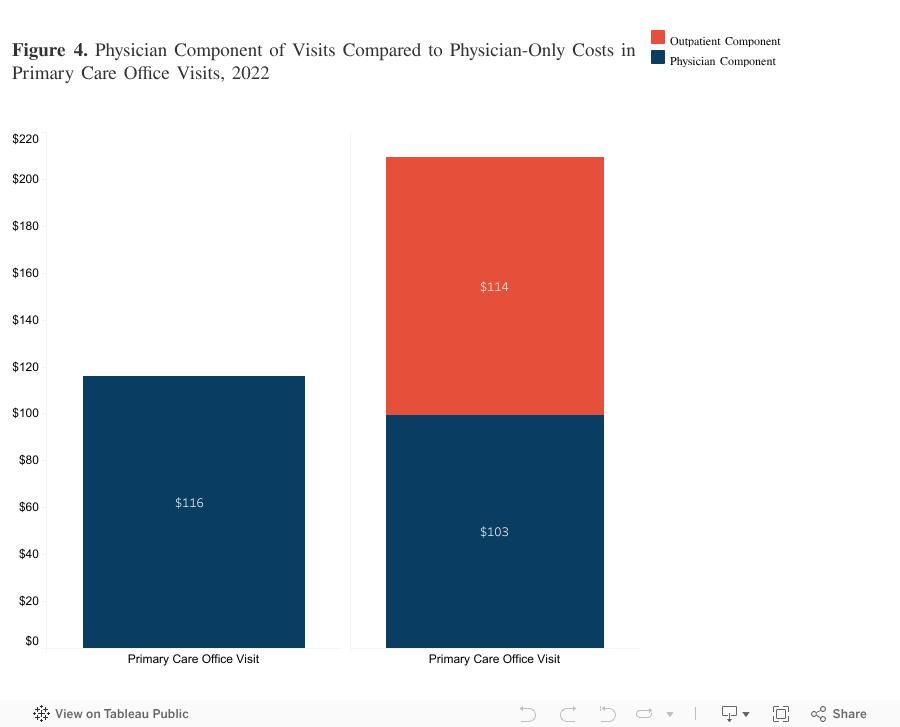
As shown in Figure 3, the physician component of visits in outpatient settings is lower, on average, than the physician-only costs. For example, as noted above, the average cost of a primary care visit in a physician office setting was $116. The physician component of a primary care office visit in an outpatient department setting was $103, a difference of $13. The facility component, however, added $114 to the total cost.
Pediatric wellness visits had a similar pattern with a physician-only cost of $144 compared to the physician component cost of $126 with an additional $114 for the outpatient facility.
Primary care office visit and pediatric wellness visit facility fees are rare but represented approximately $77 million in spending in 2022.
Even though we do observe facility fees associated with primary care and pediatric wellness office visits, the vast majority are provided in a physician’s office with no facility charge. In this analysis, we identified 0.52% of primary care visit claims that had an associated facility fee in 2022. This is such a common service, however, that the small proportion still represents a substantial number of visits. Among the entire population of people with employer-sponsored insurance, we estimate 685,000 primary care visits in 2022 had a facility fee.
Facility fees also appear to be relatively rare among pediatric wellness visits. In HCCI’s dataset, we identified only 0.36% of pediatric wellness visit claims that met our definition of facility fees. That represents 81,000 pediatric wellness visits across the entire ESI population.
As noted above, the average facility fee associated with primary care office visits and pediatric wellness visits was approximately $100. Assuming that such facility fees occur in 0.52% of primary care office visits and 0.36% of pediatric wellness visits, we estimate that nearly $77 million was spent on the facility fees that were the focus of this analysis in 2022 ($69 million on primary care office visits and $8 million on pediatric wellness visits).
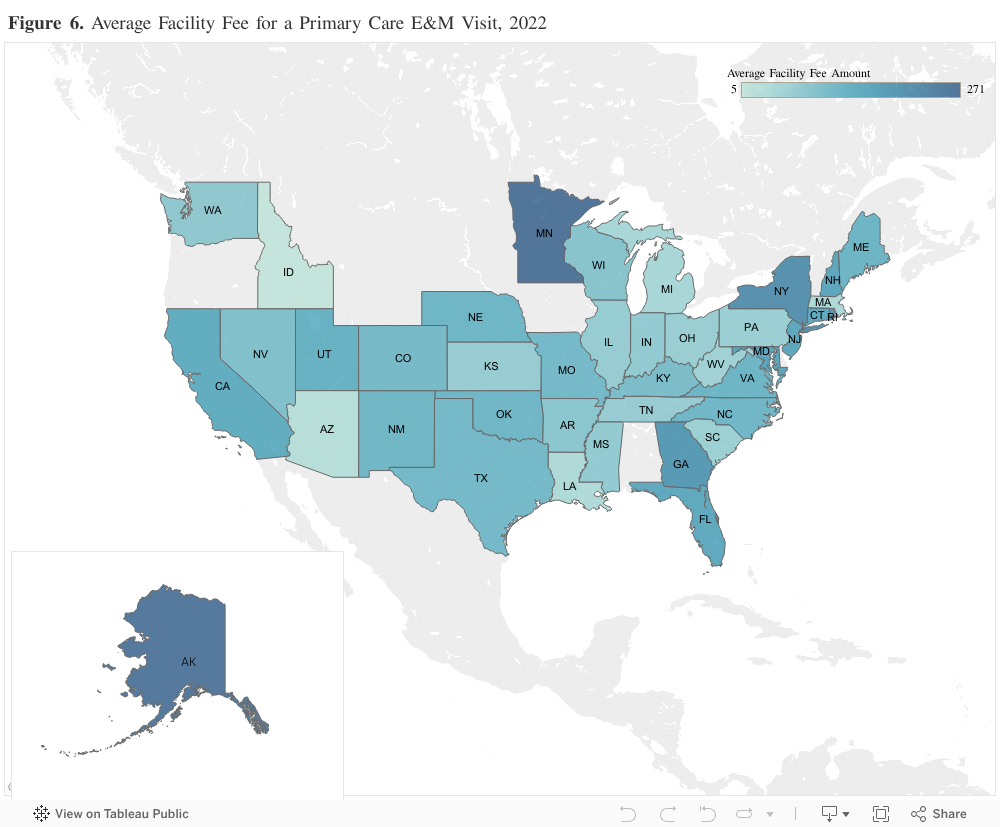
24 of 43 states study had average facility fees above $100.
Across the 43 states included in our analysis, the price of a primary care E&M visit always was higher when the visit took place in an outpatient facility than when the visit took place in a physician office. The magnitude of the price differential (referred to as ‘Facility Fee’), however, varied by state. For example, Minnesota had the largest price differential at $271, while Idaho had the smallest price differential at just $5.
It is worth noting that some state governments have taken legislative action to either restrict facility fees or increase transparency around them in recent years. As of September 2024, 18 states have passed such laws. Many of the laws prohibit providers from charging facility fees in specific instances (for example, for a telehealth visit or for preventive services), or require providers to notify patients before they receive a service that they will be charged a facility fee.
Facility Fees Can Drive Up Prices and Spending. Policymakers Look to Take Action.
This analysis focuses on primary care E&M and pediatric wellness visits, which represent just two services; many more instances of facility fees associated with office visits are possible. In fact, there may be other services where facility fees are more common than the two selected for this analysis. Taken together, the total cost of facility fees across all health care services would be substantially higher than the estimate in this analysis. As demonstrated by the examples above, facility fees drive up the prices of services. Even when the percentage of services affected is small, the aggregate impact of health care spending is large. Not only do facility fees result in higher prices in the near term, but they also create financial incentives for hospitals to acquire physician practices. Increased integration between hospitals and physician groups generally has led to higher prices for patients, employers, and insurers without improvements in care.
Some facility fees of concern to consumers and policymakers are challenging to identify in available data. Therefore, even efforts to increase transparency and disclosure of facility fees represent progress. For example, proposed federal legislation would require facilities that are associated with a hospital but are “off campus” to bill under separate identifiers from the hospital. Clear differentiation of “off campus” hospital outpatient departments will allow easier identification of facility fees on insurance claims. In addition, some states have required physician clinics that charge a facility fee to notify patients that the clinic is licensed as part of a hospital and the patient may receive a separate facility charge, resulting in higher out-of-pocket costs.
As policymakers continue to consider whether and how to address facility fees, insights into their frequency and impact will be essential.
Methodology
This analysis includes ESI claims for evaluation and management (E&M) and pediatric wellness visits that occurred in 2022 that were billed on a physician (PH) claim with place of service codes 11 (Office), 19 (Off-Campus Outpatient Hospital), or 22 (On-Campus Outpatient Hospital). Outpatient facility claims that occurred for the same patient on the same day were matched with these encounters. We excluded encounters that had a $0 outpatient facility claim line for an E&M or pediatric wellness service but had additional non-zero claim lines for other service codes for the same patient and date of service. We restricted claims to those provided by a provider with a primary care specialty, identified using the National Plan & Provider Enumeration System (NPPES) taxonomy from CMS.