
Previously, HCCI analyzed Ozempic medication use in the ESI population and found that the percentage of patients using Ozempic that had a diabetes diagnosis, the condition Ozempic is clinically indicated to treat, had decreased from 92% in 2018 to 77% 2021. This indicated a growing trend of off-label use of Ozempic. Our findings aligned with reports at the time of off-label use of Ozempic for weight loss.
Building on the previous analysis, we examined the use of 3 popular semaglutide drugs, Ozempic, Rybelsus, and Wegovy, to determine off-label use trends from 2019-2022.
The Share of Semaglutide Users without an Indicated Diagnosis Increased from 2018-2022
For each semaglutide medication, we examined the percentage of new users who did not have a diagnosis for the condition the medication is indicated to treat in the year prior to their first fill. Ozempic and Rybelsus are indicated to treat people with diabetes, and Wegovy is indicated to treat people with obesity or who are overweight. We found that the share of patients without an indicated diagnosis increased from 2019-2022 for all drugs.
Ozempic and Rybelsus
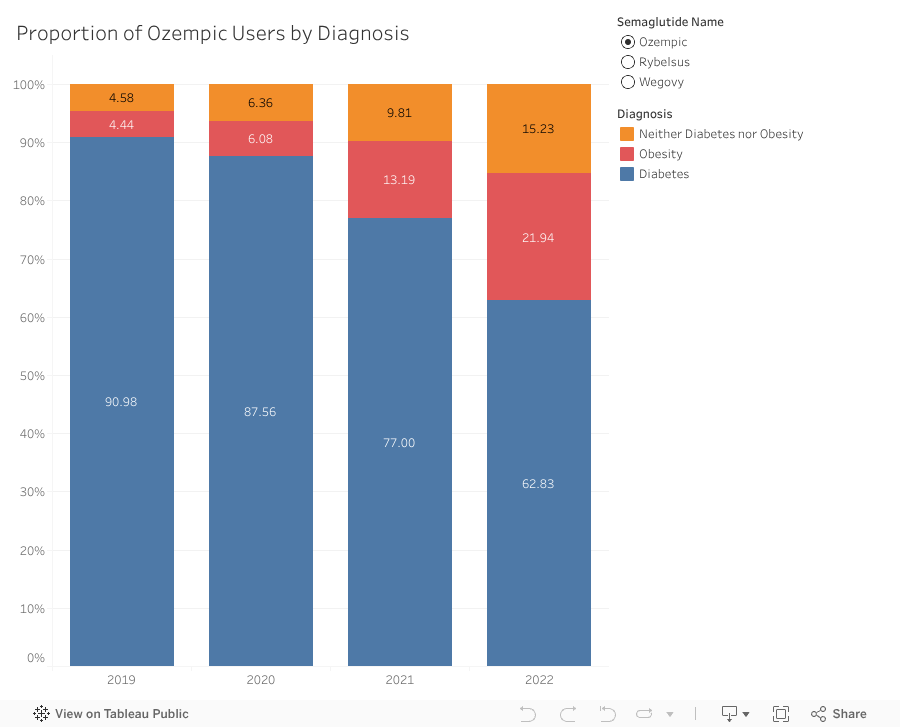
To understand the extent to which Ozempic and Rybelsus are prescribed off-label, either to treat obesity or other conditions, we stratified users by the presence of a diabetes diagnosis, obesity diagnosis without diabetes, or neither diagnosis. We found that in 2022, only 63% of Ozempic users had a documented diabetes diagnosis, down from 91% in 2019, a 31% decrease. As the proportion of Ozempic users with a diabetes diagnosis decreased, the proportion of users with an obesity diagnosis increased from 4% in 2019 to 22% in 2022, and the proportion of users without either a diabetes or obesity diagnosis increased from 5% in 2019 to 15% in 2022.
Rybelsus followed a similar pattern, though the magnitude of change over time was smaller. In 2022, 79% of Rybelsus users had a documented diabetes diagnosis, down from 86% in 2019 (an 8% decrease). The proportion of users with an obesity diagnosis increased from 5% to 10% from 2019 to 2022, and the proportion of users without either a diabetes or obesity diagnosis increased from 9% to 11% over the same period.
Wegovy
Wegovy became available in 2021 and is indicated to treat obesity or patients who are overweight with a weight-related comorbid condition, such as hypertension, type 2 diabetes, or cardiovascular disease. To analyze off-label use of Wegovy, we stratified users by the presence of an obesity or overweight diagnosis, or the absence of either diagnosis.
We found that the proportion of Wegovy users that had a documented obesity or overweight diagnosis decreased slightly from 85% in 2021 to 82% in 2022.
As Off-label Use of Semaglutides Continues to Grow, More Research is Needed on Access and Health Impacts
High levels of off-label use of any medication raise concerns about patient safety and access. One consequence of high off-label use is drug shortages. A semaglutide shortage dating back to 2022 was only resolved in early 2025. During the shortage, less regulated compound pharmacies stepped in to fill the demand for these drugs. The US Food and Drug Administration (FDA) raised concerns about compounded versions of semaglutides, citing that these drugs are not reviewed for safety, effectiveness or quality by the FDA before they are marketed, and that the agency received multiple reports of adverse effects related to dosing errors associated with compounded semaglutide products. Drug shortages make it difficult for those who need the medication to access it safely. In addition, little is known about the effects of off-label semaglutide use on patients who do not have the conditions these medications are indicated to treat. Additional studies of the effects of off-label use of semaglutides on the health of individuals and the health care system at large are warranted.
Methods Note
Our cohort includes beneficiaries who were continuously enrolled in an ESI plan for at least 1 year prior to and including the month of their first semaglutide prescription fill. For this cohort, we pulled all inpatient, outpatient, and physician claims to look for claims with a diabetes, pre-diabetes, obesity or overweight diagnosis in any diagnostic position. We counted anyone with at least 1 claim with a diagnosis in the year prior to the first semaglutide fill to have that diagnosis. This methodology has been used in prior research to identify on-label and off-label use of prescriptions.
One limitation of this analysis is that obesity and overweight diagnoses are under-recorded in claims data relative to other conditions. This may result in an overestimation of off-label use for medications indicated to treat obesity (Wegovy).