Caesarean sections (c-sections) are often life-saving procedures that can prevent injury and death among birthing people and newborns. At the same time, when they are not medically necessary, c-sections may have higher risks to babies and birthing people than vaginal births. Monitoring rates of c-sections among birthing people is an important component of efforts to improve the quality of maternal and newborn care. For example, the U.S. Department of Health and Human Services has a goal of reducing the low-risk c-section rate to 23.6% under the Healthy People 2030 objectives.
C-section rates also have a substantial impact on the health care system since they are the most common operating room procedure during an inpatient hospital stay. Moreover, there is substantial evidence, including previous HCCI work, showing that c-sections generally are more expensive than vaginal births.
In this brief, we used HCCI’s unique commercial commercial claims dataset and data from the Transformed Medicaid Statistical Information System (T-MSIS) from the Centers for Medicare and Medicaid Services to study c-section rates in ESI and Medicaid, nationally and by state.
Using both datasets, we show that more than 3 in 10 people who gave birth in the U.S. delivered their babies via c-section in 2020. At the national level, the c-section rates in ESI and Medicaid were similar (a 2.8 percentage point difference); 34% of births among people with ESI and 31% of births among people with Medicaid were by c-section. Across states, c-section rates ranged from 25% (South Dakota and Utah) to 39% (Florida) in ESI and from 22% (Alaska) to 36% (Florida and Louisiana) in Medicaid (Figures 1-2).
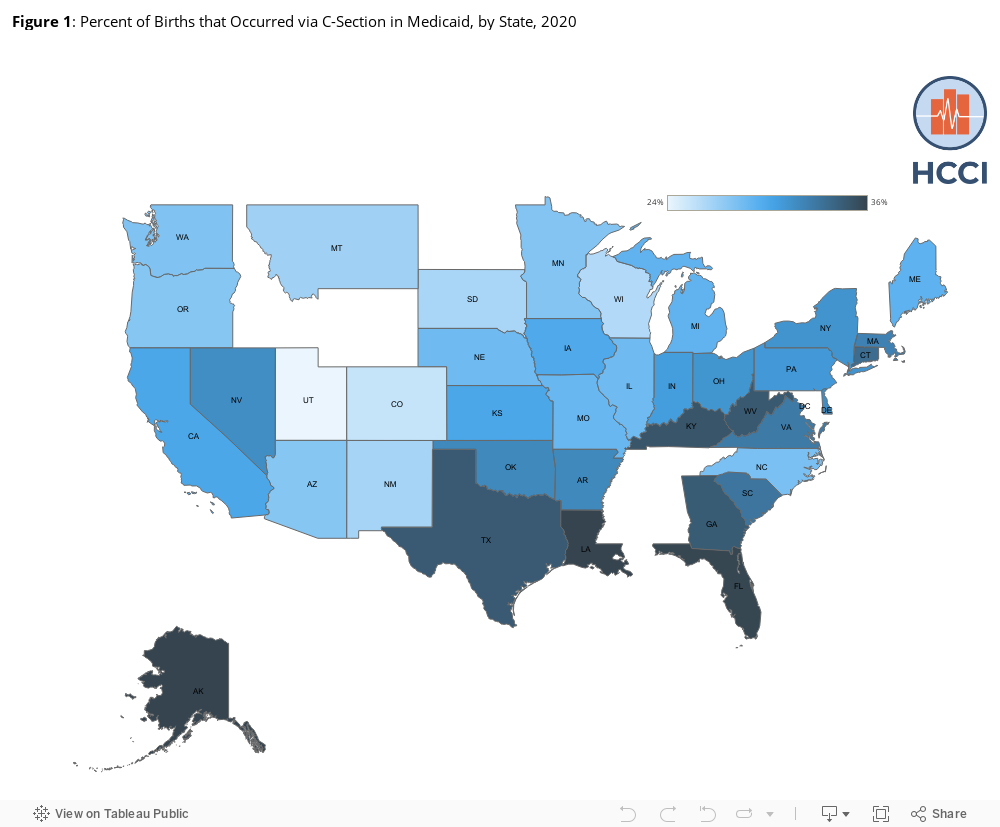
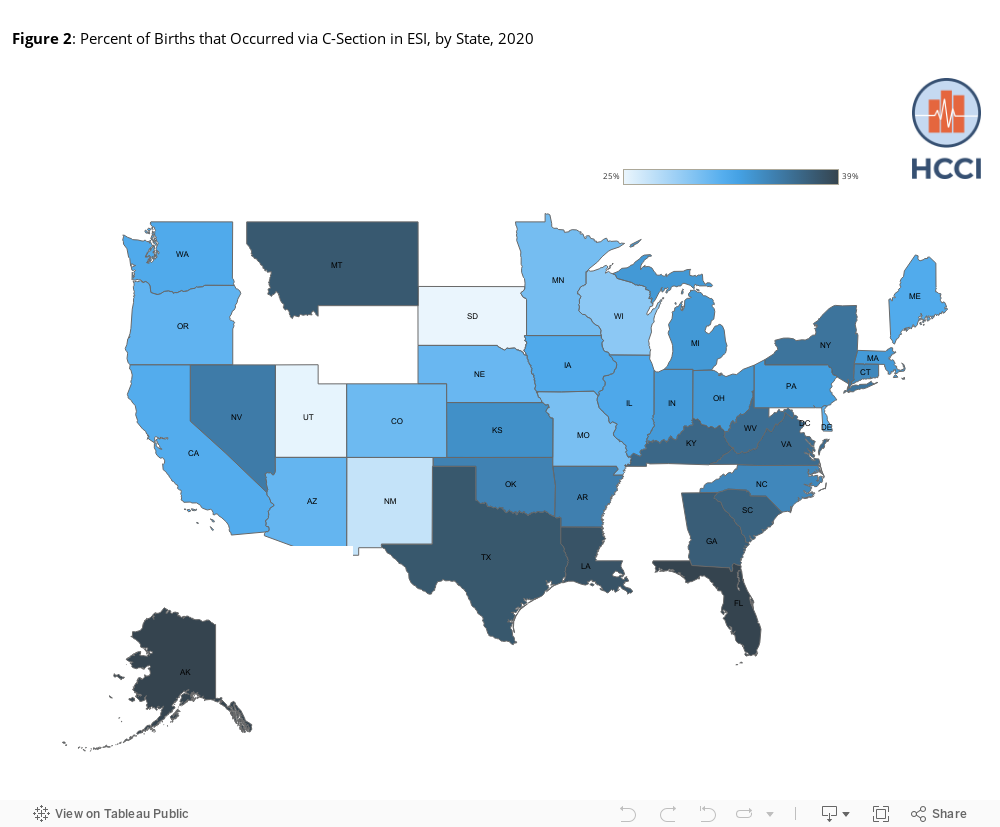
Figure 3 shows c-section rates for ESI and Medicaid in the 39 states for which we have data for both payers. States with relatively high c-section rates in ESI also have relatively high c-section rates in Medicaid. For example, Florida, where almost 40% of births occurred via c-section, is one of the states where the rates are the highest in both ESI and Medicaid. Utah, on the other hand, is one of the states where the c-section rates are the lowest (approximately 25%).

Even though c-section rates were similar, they were higher among birthing people with ESI than among those with Medicaid in 36 of the 39 states for which we have data. For the most part, differences in the c-section rates between ESI and Medicaid were small; on average, the c-section rate was 2.5 percentage points higher in ESI than in Medicaid across states. In 13 of the 36 states, the percentage point difference was less than 2.
A few states, however, did have significantly higher c-section rates in ESI than in Medicaid. In North Carolina and Alaska, for example, c-section rates were over 5 percentage points higher among birthing people with ESI than among those with Medicaid. The biggest difference in c-section rates was in Montana, where there was a 10-percentage point difference; 37% of births covered by ESI were c-sections compared to 27% in Medicaid. Three states had c-section rates in ESI that were equivalent to or slightly below the c-section rate among birthing people with Medicaid. Delaware and New Mexico, for example, had the same c-section rate in ESI and Medicaid; South Dakota was the only state where the percent of births by c-section was lower in ESI (25%) than in Medicaid (27%).
Consistent with prior evidence, our state-level findings show that c-section rates were higher in ESI than in Medicaid. Higher payments for deliveries overall, and particularly for c-sections, in ESI compared to Medicaid may incentivize overprovision of c-sections among birthing people with ESI compared to those with Medicaid. Other factors, such as the age of birthing people with ESI compared to those with Medicaid, may also contribute to higher c-section rates. For example, privately insured birthing people tend to be older than those with Medicaid and older birthing people are more likely to have a c-section than those who are younger. Social determinants and structural forces, including racism and insurance coverage, also may contribute to differences.
Safe and clinically appropriate reduction of c-sections in ESI and Medicaid has the potential to reduce birthing people’s risk and lower health care spending. Some states have introduced quality initiatives, payment reforms (e.g., coverage of doula services which have been associated with lower c-section rates), and public reporting programs with the goal of lowering unnecessary c-sections. It will be important to learn from these initiatives and scale up successful interventions to improve the outcomes of all birthing people in the U.S.
Methodology
The rate of CS is expressed as a percentage calculated by dividing the number of caesarean deliveries over the total number of deliveries. We included only enrollees who were female and between the ages of 18 and 45 years old.
In commercial claims data, we obtained a sample of more than 400,000 admissions for delivery from the 2020 inpatient delivery claims using the diagnostic information. We defined a delivery admission by the unique combination of individual, diagnostic related group (DRG), and admission and discharge dates. For state-level results, we aggregated claims at the state level and reported on states that had data on at least 400 deliveries attributed to at least five providers in 2020, including 100 vaginal birth deliveries and 100 c-section deliveries.
To the extent possible, we aimed to align methodologies across payers. In Medicaid, we examined approximately 1.4 million inpatient stays. Claims had to have an enrollment record with at least one day of eligibility in the month the delivery discharge occurred. We excluded all women who were dually eligible for Medicare and Medicaid. Less than one percent of individuals had more than one inpatient childbirth claim during the calendar year; in these cases, we kept all claims and treated each as an independent stay. DRGs were calculated using ICD-10-CM/PCS MS-DRG v37.0 definitions. The following states were excluded because the count of births in the T-MSIS claims data was more than 50% below the CDC reported Medicaid-covered births in the state: Alabama, Maryland, Mississippi, New Hampshire, New Jersey, Rhode Island, and Tennessee. Note that some states do not reconcile all or some Medicaid presumptive eligibility records, and there may be some variation in the number of records lost due to our data cleaning processes.