It is no secret that the COVID-19 pandemic upended the U.S. health care system in 2020, with effects still being felt in 2022. HCCI previously published a brief that showed precipitous drops in the utilization of several preventive health care services in early 2020. Several news outlets have also covered the effect of the pandemic on routine services, including childhood vaccination rates. The interruption of preventive care early in the COVID-19 pandemic, along with the increased utilization of telehealth appointments and virtual learning have disrupted several of the traditional methods of communication around timely routine childhood vaccinations. These factors, along with a growing wave of vaccine hesitancy predating the pandemic, have led to a decrease in routine childhood vaccinations in the U.S. compared to previous years.
To better understand this recent trend and inform public health practitioners about how best to allocate resources to increase vaccination rates, HCCI conducted an analysis of childhood vaccination trends in the U.S. from 2018-2020. Informed by administrative claims data from nearly two-thirds of the U.S. population under 18 years old, this report shows the rate of routine childhood vaccinations by year and month, stratified by type of insurance (i.e., publicly insured, including Medicaid and CHIP, or privately insured). The analysis captures approximately 56 million annual doses of vaccinations among the publicly and privately insured over the three-year period beginning January 2018.
Figure 1 shows the target age ranges and routine vaccinations used for this analysis, which follow the CDC recommended vaccination schedule.
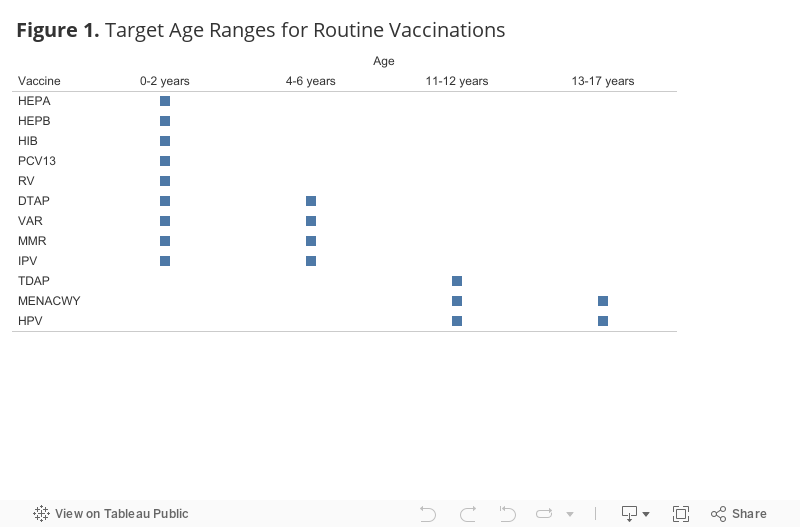
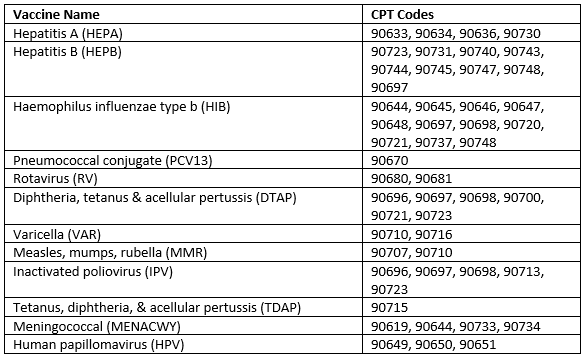
While this analysis does not examine delayed or alternative schedule vaccination timelines, our data indicate that the vast majority of routine childhood vaccines are delivered on this schedule. In this report, we focus on the following twelve routine vaccines: Hepatitis B (HEPB), rotavirus (RV), diphtheria, tetanus & acellular pertussis (DTAP), Haemophhilus influenzae (HIB), pneumococcal conjugate (PCV13), inactivated poliovirus (IPV), measles, mumps & rubella (MMR), varicella (VAR), Hepatitis A (HEPA), tetanus, diphtheria & acellular pertussis (TDAP), human papillomavirus (HPV), and meningococcal (MENACWY). Additional information on the methodology, including the data sources, can be found at the bottom of the page.
COVID-19 Disrupted On-Time Vaccination Rates in Both ESI and Medicaid Populations
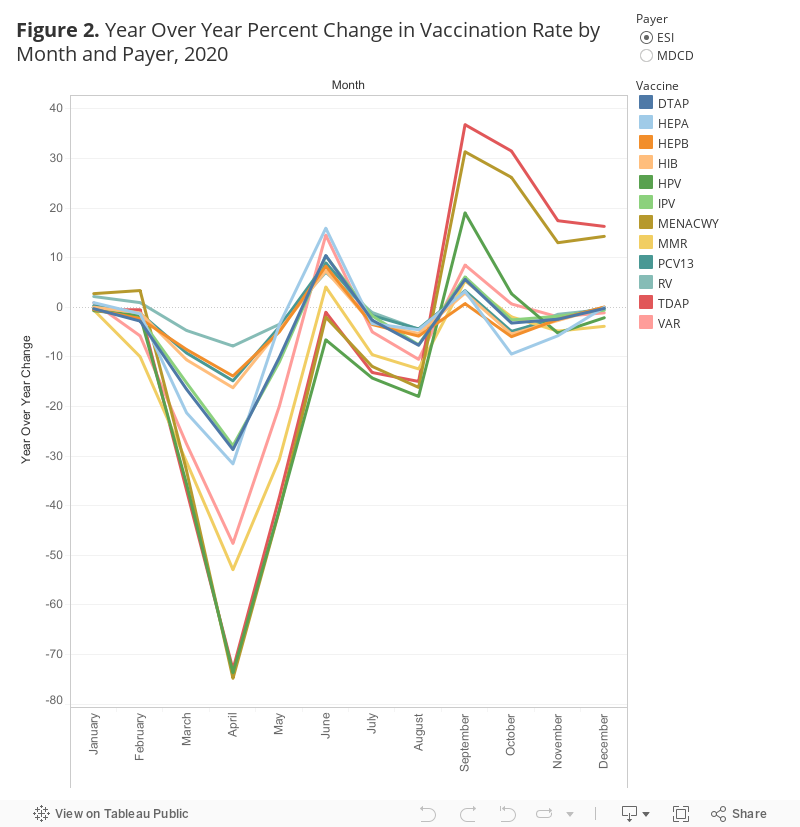
Figure 2 shows the year-over-year percent change in vaccination rate by month and vaccine in 2020. Our data show that COVID-19 disrupted on-time vaccination rates for children enrolled in both ESI and Medicaid. Vaccination rates dipped in the early months of the pandemic beginning in March 2020, as emergency orders and lockdowns were put into place. Even after COVID-19 restrictions loosened and routine health care activity was allowed to resume, some vaccination rates did not recover to the levels of previous years. Most vaccines, however, reached their pre-pandemic levels by the fall of 2020. Figure 2 can be filtered by payer for further exploration.
Overall, the difference in on-time vaccination rates between 2019 and 2020 was slightly larger among children enrolled in ESI (-6%) than enrolled in Medicaid (-4%).
- The greatest difference in on-time vaccinations between 2019 and 2020 among children enrolled in ESI were HPV, which decreased by over 14%, and MMR, which decreased by more than 13% from 2019. The remaining vaccine rates all decreased by between 1%-8%.
- Among children enrolled in Medicaid, the HPV vaccine rate also saw a large drop (decreasing by over 18% from 2019), and the meningococcal vaccination rate decreased by nearly 14% from 2019. The Hepatitis B, HIB, PCV13 and rotavirus rates all increased by about 1% or less in 2020 compared to 2019. The remaining vaccine rates all decreased by between 2%-11%.
Vaccination Rates for School-Aged Children Peak Before the Start of the School Year
Irrespective of the trends observed in 2020, in all three years, rates for vaccinations that are recommended for school aged children (ages 4-17) peaked during July and August. For example, the meningococcal vaccine, recommended for adolescents aged 11-17, typically has a rate of around 1,000 per 100,000 in April, but it increases dramatically during the summer months, culminating in rates 2-4 times higher at their apex in August. This trend is visible in both ESI and Medicaid. It is likely that this late-summer peak is due to vaccination requirements enforced by public schools, which usually begin the school year in late August and early September.
During the height of the pandemic, rates for vaccines that occur within the first year of life decreased less than those for older children. It appears that on-time vaccination rates among the youngest age group, such as Hepatitis B, HIB, PCV13, and rotavirus, were less affected by the pandemic compared to vaccines that occur or have subsequent doses after the first year.
Vaccination Rates Decreased Disproportionately in Specific States in 2020 Compared to 2019
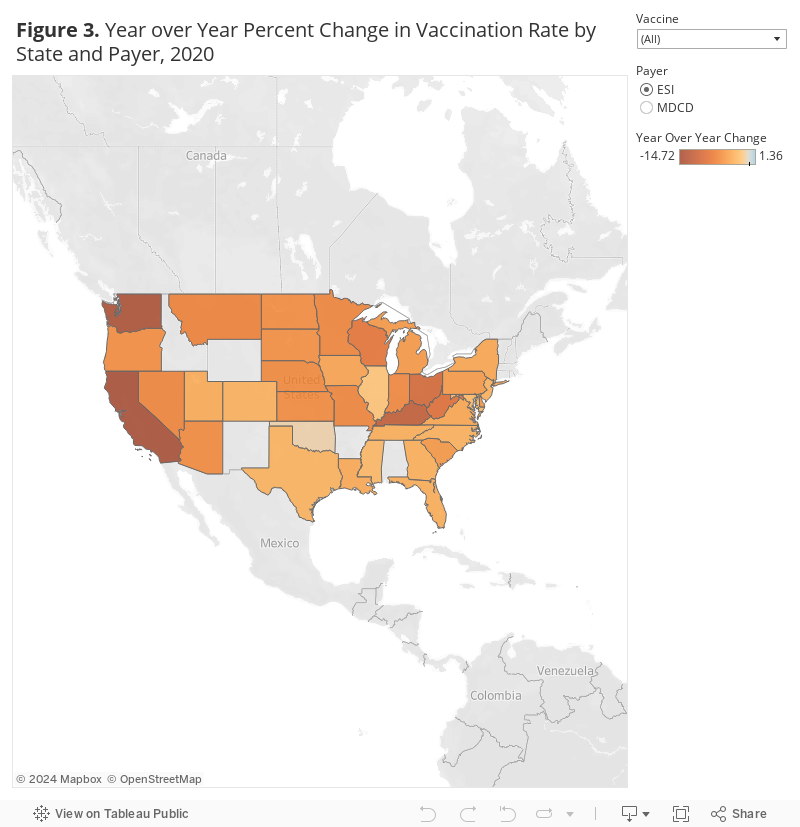
Figure 3 shows the year over year percent change in vaccination rate by state and payer in 2020. Our data show that vaccination rates changed differentially among states in 2020 compared to 2019.
Among children enrolled in ESI, the largest decreases in overall vaccination rates occurred in California (-15%), Washington (-14%), Kentucky (-12%), Ohio (-10%), and West Virginia (-9%). Only one state, Hawaii, experienced an increase in their overall vaccination rate from 2019 to 2020.
- In California, the largest drop occurred in the MMR vaccine rate (-27%); the RV vaccination rate (-5%) saw the smallest decline.
- In Hawaii, the TDaP vaccination rate decreased the most from 2019 to 2020 (-5%), while the Hepatitis A vaccination rate increased the most (15%).
Among children enrolled in Medicaid, the largest decrease in overall vaccination rate occurred in Wisconsin (-17%), followed by Michigan (-16%), Oregon (-15%), Louisiana (-14%) and Maryland (-14%). In contrast, in several states, the overall vaccination rate among children enrolled in Medicaid increased in 2020, including Wyoming (24%), Indiana (24%), Georgia (21%), Nebraska (15%) and Alabama (11%). Note that the Medicaid data is still preliminary, and some states may revise the claims submissions later in the year.
- In Wisconsin, the decrease in the Medicaid HPV vaccination rate was the largest (-28%); the vaccine with the smallest decrease was Hepatitis B (11%).
- In Wyoming, no vaccination rates decreased, and the HIB vaccination rate increased the most (57%).
Data Highlights Need for Public Health Efforts to Increase Childhood Vaccinations in both the ESI and Medicaid Populations
HCCI’s data show that, in 2020, on-time vaccination rates decreased significantly compared to previous years. The decrease in overall vaccinations rates was slightly higher among children enrolled in ESI than those enrolled in Medicaid. The extent of the decrease, however, varied by state and vaccine type. The pandemic appears to have had a smaller impact on vaccinations for younger children (0-2 years old) than older children (ages 4+). This could be because infants had more contact with the health care system in the first year of life despite the pandemic, receiving more routine care and checkups than older children and adolescents. Increase contact with the health care system may increased their likelihood of receiving on-time vaccinations. Our data also show that annual peaks in vaccination rates for certain vaccines coincide with the start of the school year, which may indicate that school vaccination requirements are an effective tool to promote vaccination. The trends we see in our data highlight the need to continue research on vaccination rates in the years following the pandemic, as well as to uncover drivers of disparities in vaccine access.
We used administrative claims records to measure changes in vaccination rates for children enrolled in public and private health insurance plans. Although these data help point to overall trends in vaccine utilization, there are a few limitations. This approach leaves out the uninsured and may also not represent the underinsured. For example, claims submission guidelines under the Vaccines for Children (VFC) program may mean that many children who do get vaccines, particularly those in households with lower incomes, are not included in claims data. State vaccine registries remain the best sources of data for targeting individuals and groups for vaccine information intervention for these reasons.
Methods Note
The vaccination rates were calculated as the total number of vaccinations amongst the eligible population divided by the total eligible population per 100,000 enrollees. Eligibility in the numerator and denominator was determined based on the CDC recommended age for on-time vaccinations. The recommended age varies by vaccine (see Figure 1).
In our ESI claims data, patient-level date of birth is not available, so we calculated an approximate age based on year of birth. We calculated age as reporting year minus the year of birth.
We were not able to directly compare rates across payers for a few reasons, including the different state-level policies regarding the administration of the national Vaccines for Children (VFC) program, as well as missing data due to other state programs that provide vaccinations free of charge, which often do not generate claims data. Some states were excluded from the analysis due to the aforementioned reasons.
The following states were excluded from our ESI analysis: Maine, Vermont, New Hampshire, Massachusetts, Connecticut, Rhode Island, Alabama, Arkansas, New Mexico, Wyoming, and Idaho.
The following states were excluded from our Medicaid analysis: Vermont, Rhode Island, Pennsylvania, New Jersey, West Virginia, Tennessee, Oklahoma, Colorado, and Arizona.
The CPT codes used in this analysis are as follows: