
Every year, 1 million people in the U.S. receive chemotherapy for cancer treatment. Most chemotherapy treatment requires patients to be present in a physician’s office or hospital outpatient department to receive the treatment (typically an infusion or injection). Chemotherapy plays a critical role in treatment for many patients with cancer, but it also often leads to high financial costs for patients and their families. In addition to the high costs of many chemotherapy medications themselves, where patients receive their treatment (e.g., in a physician’s office or a hospital outpatient department) may have meaningful implications for how much they pay.
Previous HCCI work has shown that outpatient services cost patients and insurers substantially more than the same services provided in a physician’s office. We have also found that a growing share of many services (e.g., labs, drug administration, imaging) is provided in outpatient departments over time. Therefore, by choosing a particular physician or health system for treatment, patients may unknowingly be exposed to higher costs just by virtue of whether the care is provided in an outpatient department or a physician’s office.
This analysis shows an increasing share of chemotherapy services provided in outpatient departments between 2014 and 2020. As with other services, this analysis also finds that chemotherapy costs more in outpatient settings compared to physician offices. We focus specifically on the population with health insurance through an employer (employer-sponsored insurance, or ESI) using the Health Care Cost Institute’s dataset of health care claims for about one-third of the ESI population.
Over Half of Chemotherapy was in Outpatient Departments in 2020, up 25% from 2014
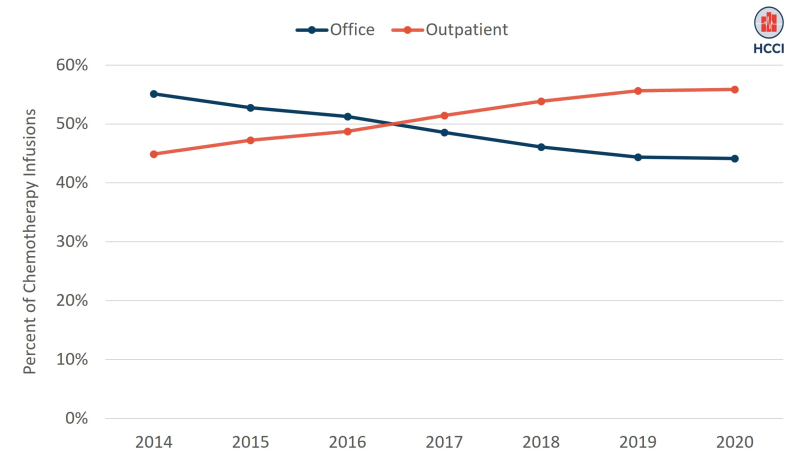
We identified instances of infused chemotherapy treatment in the HCCI data based on Healthcare Common Procedure Coding System (HCPCS) codes in professional and facility claims from 2014-2020. Consistent with earlier work, this analysis finds that the share of chemotherapy provided to people with ESI in outpatient departments has increased over time. By 2020, more than half of all chemotherapy infusions—56%—were provided in outpatient departments. That reflects 25% growth from 2014 to 2020, as shown in Figure 1.
Figure 1. Over Half of Chemotherapy in the HCCI Data was Provided in Outpatient Settings in 2020
Total and Out-of-Pocket Costs were Higher for Outpatient Chemotherapy than for Office-Based Chemotherapy
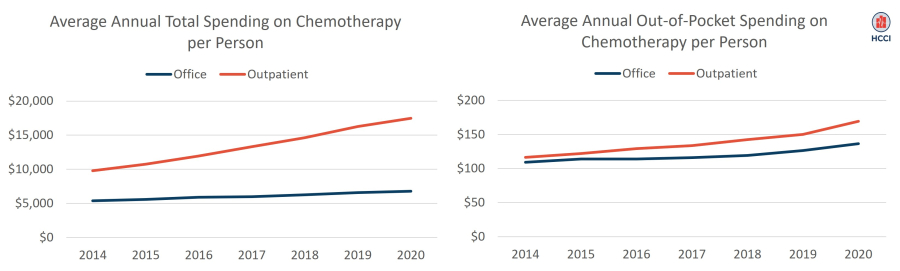
As shown in Figure 2 (left panel), average annual per person total spending (i.e., allowed amount) for chemotherapy was higher for outpatient-based chemotherapy than office-based chemotherapy in all years. For example, in 2020, average spending on outpatient-based chemotherapy was $17,493 compared to $6,775 for office-based chemotherapy.
Between 2014 and 2020, per person spending on chemotherapy rose for all patients with chemotherapy but grew substantially more for those receiving treatment in outpatient settings than for those receiving treatment in a physician’s office. Spending for outpatient-based chemotherapy grew close to 80% from 2014 to 2020, from just under $10,000 to $17,493, while per person spending for office-based chemotherapy grew 26%, from $5,377 to $6,775.
Differences in spending for outpatient chemotherapy may reflect a different mix of chemotherapies provided in outpatient settings compared to office settings as well as higher prices for the same drugs in these departments than in physician offices. For example, the most common chemotherapy drug in our data, fluorouracil, cost $138 on average per dose (i.e., patient-service day) in an outpatient department compared to $30 on average in a physician’s office.
Patient out-of-pocket spending on chemotherapy (Figure 2, right panel), defined as total out-of-pocket spending on chemotherapy services divided by the number of patients with a chemotherapy claim in a given calendar year, was similar across outpatient and office settings but still higher for outpatient treatment than for office-based treatment in all years. In 2020, patients paid, on average, $169 out-of-pocket for outpatient chemotherapy and $136 for office-based chemotherapy.
The similarity in out-of-pocket spending across settings, as well as the amount of payment, are likely reflective of health insurance benefit design controlling how much people spend out-of-pocket. Other evidence has shown that chemotherapy costs are a relatively small proportion of total out-of-pocket costs among people with cancer; in many cases, patients may reach their out-of-pocket maximum in the early months of diagnosis (e.g., due to surgery) and then be protected from additional cost-sharing during the year.
Though out-of-pocket spending is relatively similar across outpatient departments and physician offices, it increased more for outpatient chemotherapy than for office-based chemotherapy between 2014 and 2020 (45% compared to 25%). Therefore, as shown in Figure 2, the differential in out-of-pocket spending between outpatient and office chemotherapy has grown over time.
Figure 2. Annual per Person Spending on Chemotherapy in HCCI Data, 2014-2020
Site Neutrality Could Help Lower Costs for People Receiving Chemotherapy
Costs associated with chemotherapy are just one component of the myriad financial costs that patients with cancer and their families face, which may also include costs associated with hospital and emergency care, medical appointments, imaging, and prescription drugs, as well as loss of wages and caregiving needs. Even compared to other patients with health care debt, patients who had cancer (or an immediate family member with cancer) were more likely report that they skipped or delayed medical care due to cost, used up most of their savings, or declared bankruptcy or lost their home due to eviction or foreclosure.
In some cases, the financial strain associated with cancer treatment has been associated with worse quality of life and even higher mortality risk. Patients who are in minoritized racial/ethnic groups are more likely to experience financial hardship associated with cancer care, driven by a variety of systemic and clinical factors, including a higher likelihood of being diagnosed at later disease stage and of receiving inappropriate treatment.
Chemotherapy is associated with higher and faster-growing spending when provided in outpatient departments compared to physician offices. Though patients may be insulated from these costs to a certain extent by their insurance, higher spending raises costs for employers and insurers and indirectly affects patients through premiums, wages, and other forms of compensation. Our data show that the share of chemotherapy occurring in outpatient departments compared to physician offices increased from 2014 to 2020, with more than 50% of all chemotherapy services provided in outpatient departments by 2020.
Payment differences across sites of care expose patients to higher costs, in many cases without meaningful changes in quality of care. In addition, these differentials incentivize further consolidation, including, for example, hospital acquisition of physician offices, which is associated with higher prices. Medicare is moving towards equalizing payments across sites of care for services that can be safely provided in non-hospital settings, and MedPAC has identified drug administration, such as infused chemotherapy, as one such service. Employers and insurers providing ESI may consider expanding use of site neutral payment for chemotherapy to reduce spending and financial burden on patients.
Methods
We restricted our analysis to adjudicated outpatient facility and professional claims with an employer-sponsored insurer health plan as the primary payer and allowed amounts greater than $1 between 2019 and 2021. We classified claims as office setting if a claim has a place of service of 11 and claims as outpatient department setting if a claim has a place of service of 19 or 22. We identified chemotherapy HCPCS code using BETOS crosswalk and excluded chemotherapy administration codes from our analysis.