Inequities in health care access and outcomes among vulnerable populations are well-documented, as is the fact that where you live affects health outcomes to a similar or even greater extent than your health behaviors. Previous HCCI work shows that employer-sponsored health insurance (ESI) plays an important role in many vulnerable communities. Among the population in the United States with health insurance, most people who live in socially vulnerable and rural areas are covered by ESI. Therefore, we used HCCI's commercial claims dataset, which covers about one-third of people with ESI, to understand more about disparities in health care access and outcomes within this population.
Our data show that prevention and screening services are generally utilized less in rural areas and more socially vulnerable areas compared to urban and less socially vulnerable areas. Disease management does not vary between rural and urban areas, though more socially vulnerable areas have lower rates of medication adherence compared to less socially vulnerable areas. This analysis generally follows CMS and HRSA definitions of "rural" and "urban," classifying zip codes with a rural-urban commuting area (RUCA) classification of 1-3 as urban and areas with a classification of 4-10 as rural. Social vulnerability is as measured by the CDC's Minority Health-Social Vulnerability Index (MH-SVI).
We examined utilization of several common services in the following broad categories:
- Prevention. We examined childhood vaccines (Measles-Mumps-Rubella [MMR], Human Papillomavirus [HPV]) to gauge differences in prevention. We measured vaccination rates per 100,000 enrollees, restricted to the appropriate age and sex groups.
- Screening. To assess whether there were disparities in screening, we examined mammography, colonoscopy, and prostate-specific antigen [PSA] testing. As with vaccines, we measured cancer screening rates per 100,000 enrollees, restricted to the appropriate age and sex groups.,
- Treatment. We relied on measures of disease management for insights into treatment services. Specifically, we looked at medication adherence for hypertension and for asthma. We calculated hypertension medication adherence as the percent of those with diagnosed hypertension and two fills for associated medications who had at least 80% of days covered with medication. We measured asthma medication adherence as the percent of those with diagnosed asthma who had at least half of their associated prescription fills for controller medications rather than reliever medications.
Prevention and Screening were Generally Lower in Rural Areas Compared to Urban Areas while Medication Adherence Rates were Similar
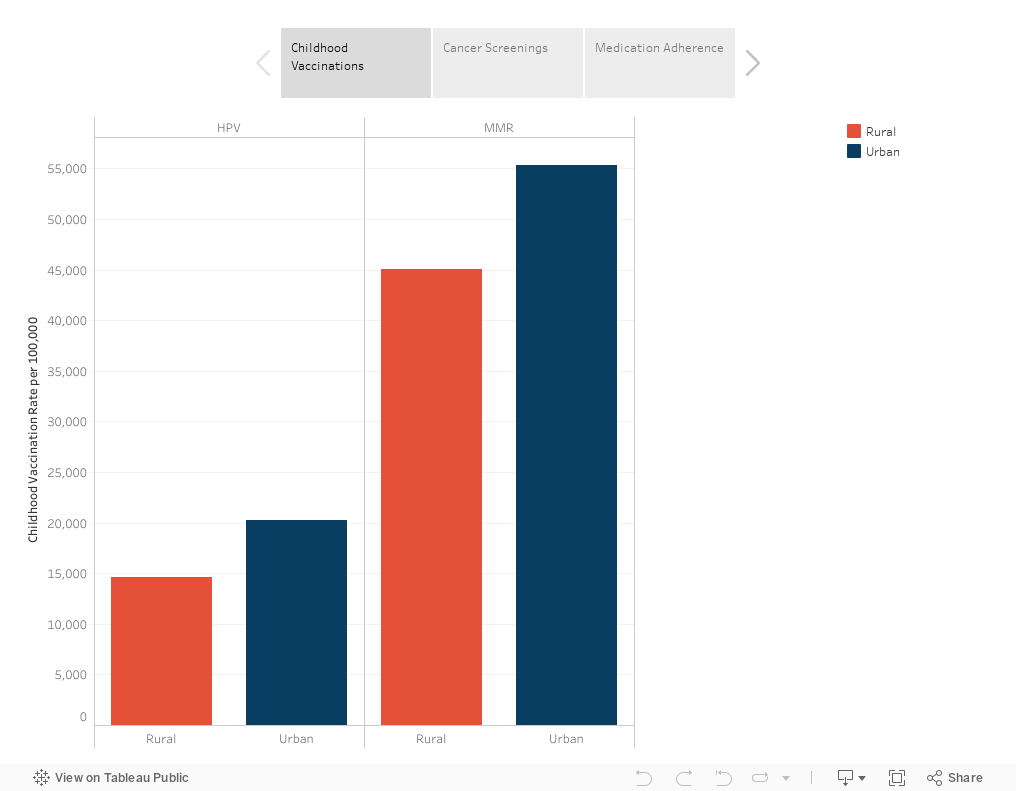
We find that vaccination and screening rates were around 20% lower in rural areas than in urban areas (Figure 1). For example, MMR vaccination rates were 19% lower in rural areas (45,097 per 100,000) than urban areas (55,341 per 100,000), and HPV vaccination rates (14,670 per 100,000) were 28% lower (14,670 per 100,000 and 20,284 per 100,000, respectively).
Similarly, in the case of each of the cancer screenings we looked at, rates were more than 20% lower in rural areas than in urban areas (Figure 1). We observed the largest difference in rates of PSA tests, which were 30% lower in rural areas (20,822 per 100,000) compared to urban areas (29,612 per 100,000).
Unlike vaccinations and cancer screenings, we found similar rates of medication adherence for both hypertension and asthma in rural and urban areas (Figure 1). Hypertension medication adherence rates were about 76% in both urban and rural areas while asthma medication adherence rates were about 70% in both urban and rural areas.
The small differences we observe in medication adherence rates may be because adherence rates are based on people who are fairly engaged with the health care system. Specifically, adherence measures were calculated as a percentage of people with a diagnosis of the disease and who have at least 1-2 prescription fills. Thus, people who may not have access to health care services are not included in the measure. While these restrictions are needed to reliably calculate medication adherence, they also mean that our measures likely do not fully capture the disparity in appropriate care for these chronic conditions in rural compared to urban areas.
Moreover, people in rural areas with ESI coverage are unlikely to be representative of everyone who lives in rural areas. Many people in rural areas who are enrolled in ESI are, by definition, working and working in a firm that offers health insurance; therefore, the population in our data may systematically differ from the broader rural population.
Figure 1. Vaccination, Screening, and Medication Adherence Rates among ESI Enrollees in Urban compared to Rural Areas (2020)
Prevention, Screening, and Medication Adherence Rates were Lowest in the Most Socially Vulnerable Areas
To measure social vulnerability, we used the Minority Health Social Vulnerability Index (MH-SVI), developed by the CDC and HHS Office of Minority Health. We calculated the MH-SVI for each zip code and divided zip codes into quintiles based on their score, such that a quintile equal to 1 represented the least vulnerable zip codes and a quintile equal to 5 represented the most vulnerable zip codes.
All the preventive, screening, and adherence rates we studied were lower in more socially vulnerable zip codes (Figure 2). The greatest disparity between the least and most vulnerable zip codes was in childhood vaccinations. The MMR rate was close to 30% lower in the most vulnerable areas than in the least vulnerable areas (45,232 per 100,000 compared to 62,970 per 100,000), and the HPV vaccination rate was 43% lower in the most vulnerable areas than the least vulnerable areas (14,713 per 100,000 compared to 26,018 per 100,000).
Cancer screening rates were more than 20% lower in the most vulnerable zip codes, compared to the least vulnerable zip codes. For example, mammography rates were 24% lower in the most vulnerable areas compared to the least vulnerable areas (34,256 per 100,000 compared to 45,033 per 100,000). Differences in medication adherence were smaller between areas that were classified as more versus less vulnerable. Hypertension medication adherence was 11% lower in the most vulnerable areas, while asthma medication adherence was 7% lower in the most vulnerable areas compared to the least vulnerable areas.
Figure 2. Vaccination, Screening, and Medication Adherence Rates among ESI Enrollees by Quintile of MH-SVI Index Value (2020)
Across MH-SVI Themes, Vaccination and Screening Rates were Generally Lower in More Vulnerable Areas, with Smaller Differences in Medication Adherence
The MH-SVI is an index, consisting of measures grouped into six themes:
- Socioeconomic status
- Housing and transportation
- Medical vulnerability
- Health care access
- Household composition, and
- Minority status and language
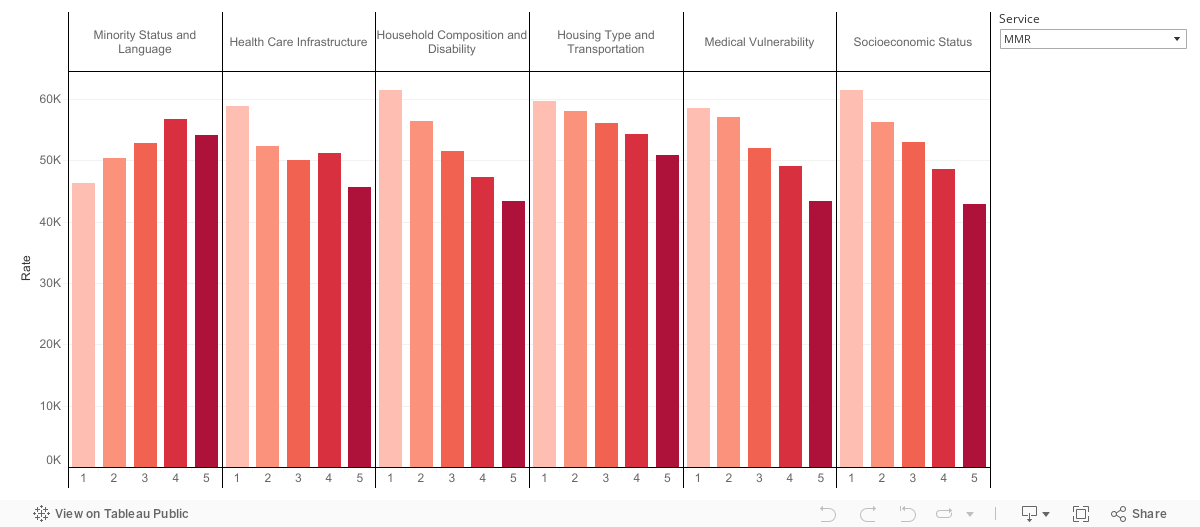
To better understand what drives the variation across areas with different overall MH-SVI levels, we examined rates of our measures of interest by quintile for each theme (Figure 3).
Consistent with the overall MH-SVI, childhood vaccination and cancer screening rates among the ESI population were lower in more vulnerable communities as captured by five of the six MH-SVI themes (all other than minority status and language). As with the composite MH-SVI, differences between the most and least vulnerable MH-SVI quintiles were largest for childhood vaccinations, with rates in the most vulnerable areas that were at least 15% lower than rates in the least vulnerable communities.
In contrast to the overall MH-SVI and the other themes, people living in more vulnerable areas with respect to the minority status and language theme generally had higher rates of vaccination and screening compared to people living in less vulnerable areas. Zip codes in the highest vulnerability quintile for minority status and language had rates that ranged from a similar level (e.g., for colonoscopy and mammography screenings) to 20% above (e.g., for HPV vaccinations) rates in zip codes in the lowest vulnerability quintile of this dimension of MH-SVI.
The different patterns observed for the minority status and language theme are likely because over 95% of areas that are classified as most vulnerable according to the minority status and language theme are urban, and these areas (as shown earlier) have higher rates of vaccination and screening than areas classified as rural.
In keeping with results presented in the earlier sections, we generally observed relatively small disparities in medication adherence across MH-SVI themes. Medication adherence was lower among zip codes that were classified as more vulnerable in terms of socioeconomic status, housing type and transportation. Medication adherence rates were similar among zip codes that were classified as more vulnerable in the other three themes: minority status and language, health care infrastructure and access, and household composition and disability.
Although vaccinations and screenings were higher in areas classified as more vulnerable based on minority status/language, medication adherence rates were (modestly) lower in these areas. For example, hypertension medication adherence was 72% in the least vulnerable zip codes as measured by the minority status and language MH-SVI theme, compared to 68% in the most vulnerable zip codes. As discussed earlier, differences in medication adherence across this dimension may be related to the nature of these measures (i.e., they are measured in a subset of the population that has a diagnosis and at least one prescription fill, so require more interaction with the health care system than other measures).
Figure 3. Vaccination, Screening, and Medication Adherence Rates among ESI Enrollees by Quintile of MH-SVI Theme Value (2020)
Place-Based Measures Combined with Claims Data Show Disparities within the ESI Population in Prevention, Screening, and Treatment
This analysis highlights gaps in use of common preventive and screening services both in rural and more socially vulnerable areas. One measure of treatment—disease management—saw smaller disparities.
Our data provide a look at place-based disparities in common preventive services and treatment and reveal that, even within the ESI population, we observe meaningful disparities in utilization and access to care. The ability to link place-based measures of health and social vulnerability to claims data is an important tool for examining and uncovering drivers of disparities. In particular, the MH-SVI and rural analyses allow us to take a more of a holistic view of the many interacting variables that affect a person's wellbeing and access to health care.
These findings improve our understanding of the ESI population, which has value for researchers as well as policymakers, employers, and payers who are engaged in this market and aim to improve equity in access to health care and health outcomes in this population.
Detailed Methodology
Rurality
- Urban includes RUCA Codes 1-3:
- 1: Metropolitan area core (primary flow within an urbanized area)
- 2: Metropolitan area high commuting (primary flow 20% or more to an urban area)
- 3: Metropolitan area core (primary flow 10% to 30% to an urbanized area)
- Rural includes RUCA Codes 4-10:
- 4: Micropolitan area core (primary flow within an urban cluster of 10,000 to 49,999 (i.e., a large urban cluster))
- 5: Micropolitan high commuting (primary flow 30% or more to large urban cluster)
- 6: Micropolitan low commuting (primary flow 10% to 30% to large urban cluster)
- 7: Small town core (primary flow within an urban cluster of 2,500 to 9,999 (i.e., a small urban cluster)
- 8: Small town high commuting (primary flow 30% or more to a small urban cluster)
- 9: Small town low commuting (primary flow 10% to 30% to a small urban cluster)
- 10: Rural areas (primary flow to a tract outside an urban area or urban cluster)
Social Vulnerability
- We measure social vulnerability using the CDC's Minority Health Social Vulnerability Index (MH-SVI). The MH-SVI consists of the following measures, which are drawn from the U.S. Census American Community Survey. The MH-SVI includes a composite score and individual scores for each of the six themes:
- Socioeconomic Status: % Below poverty, % Unemployed, Per capita income, % No HS Diploma
- Household composition and disability: % aged 65+, % aged <18, % older than age 5 with a disability, % single parent households
- Minority status and language: % minority (individual measures for American Indian/Alaska Native, Asian, African American, Native Hawaiian/Pacific Islander, Hispanic or Latinx, Some Other Race), % speak English less than "very well" (individual measures for Spanish speakers, Chinese speakers, Vietnamese speakers, Korean speakers, Russian speakers)
- Housing Type and Transportation: % multi-unit structures, % mobile homes, % crowding, % no vehicle, % group quarters
- Health Care Infrastructure and Access: # of hospitals, # urgent care clinics, # pharmacies, primary care physicians per 100,000, % uninsured
- Medical Vulnerability: % households with no internet access, prevalence cardiovascular disease, prevalence Chronic respiratory disease, prevalence obesity, prevalence diabetes
HEALTH MEASURES
Childhood Vaccination: HPV and MMR Rates
- We measured childhood vaccination rates using HPV and MMR rates per 100,000. Service counts were determined using professional claims, counting unique claim dates for each patient and vaccine. These measures show the number of enrollees in the eligible population that received the vaccine per 100,000 enrollees.
- The eligible population for each measure was restricted to the relevant age groups:
- MMR vaccinations include enrollees 0-2 years old and 4-6 years old
- HPV vaccinations include enrollees 11-17 years old
- We excluded areas (zip codes) with state and community-level free vaccine drives since vaccines delivered in these settings do not show up in claims, resulting in an undercount in claims data.
- We selected MMR and HPV because they cover different age groups and while MMR vaccinations are well-established and typically required for children to enroll in public schools, HPV vaccinations are newer and are only required for public school enrollment in four U.S. jurisdictions.
- Therefore, looking at both vaccines gives us a sense of vaccination rates across a broad population, and whether patterns of vaccination across different types of areas vary across age groups.
Cancer Screening: Mammography, Colonoscopy, and PSA Rates
- We measured cancer screening rates using mammography, colonoscopy, and prostate-specific antigen (PSA) rates per 100,000. These measures show the number of enrollees in the eligible population (this restricts the population to the relevant age range and sex) that received a screening per 100,000 enrollees.
- Measures are restricted to the appropriate age and sex groups:
- The population for colonoscopy includes male and female enrollees between ages 45 and 64
- The population for mammography is restricted to female enrollees between 45 and 64 years old
- The population for PSA is restricted to male enrollees between 45 and 64 years old
- These cancer types are among the five most prevalent cancers in the U.S., and therefore can provide information on cancer screening for a broad population.
- Each of these cancer types is relevant to different age and sex groups, enabling us to determine whether there is variation in health care use patterns across different populations within the same area, by social vulnerability and rurality.
Medication Adherence: Asthma and Hypertension
- To measure asthma medication adherence, we used the Asthma Medication Ratio (AMR) HEDIS measure. This measure identifies individuals with persistent asthma and at least one fill of an asthma medication who had a ratio of controller medications to total asthma medications of 0.50 or greater during the measurement year.
- To measure hypertension medication adherence, we adapted from methodology of a performance metric developed by the Pharmacy Quality Alliance (PQA). Our measure identifies a cohort of individuals diagnosed with hypertension and who had at least two fills of renin angiotensin system antagonists (RASAs). RASA medication adherence is defined as meeting a threshold of 80% or higher in the percent of days in the measurement period that were "covered" by RASA prescription claims during the calendar year after they received a diagnosis. A version of this measure was adapted by CMS in their Medicare Part D Star Ratings system and is endorsed by the National Quality Forum.
- Medication adherence rates only account for individuals who have already had an encounter with the health care system; therefore, some individuals with the applicable conditions (asthma or hypertension) may not be included in the measure population.
- Hypertension is more common among and adult population, while asthma is more common among children. Therefore, examining hypertension and asthma medication adherence allow us to analyze the extent to which adult and children are receiving appropriate treatment for managing chronic conditions across different neighborhoods.
- Hypertension and asthma medication adherence measures provide a benchmark for treating chronic diseases with high and varying prevalence across different populations given evidence that there are large socioeconomic and racial and ethnic disparities in the prevalence of hypertension and asthma.